Gait And Gait Aids
GAIT CYCLE
The normal gait cycle has two primary components: stance phase, which represents the duration of foot contact with the ground, and swing phase, which represents the period in which the foot is in the air. The typical gait pattern consists of approximately 60% stance phase and 40% swing phase. Figure 2-1 shows the components of gait.
A Step is defined as the time measured from an event in one foot to the subsequent occurrence of the same event in the other foot.
A Stride is defined as the time measured from an event in one foot to the subsequent occurrence of the same event in the same foot.
THE SIX DETERMINANTS OF GAIT
Saunders et al.1 began by assuming that gait is most efficient when vertical and lateral excursions of the body’s COG are minimized. They identified six naturally occurring “determinants” in normal gait that reduced these excursions and suggested that pathologic gait could be identified when these determinants were compromised.
1. Pelvic rotation in the horizontal plane – The pelvis rotates 4° to each side, which occurs maximally during double support, elevating the nadir of the COG pathway curve by about 3/8”.
2. Pelvic tilt in the frontal plane – The pelvis drops 5° on the side of the swinging leg controlled by the hip abductors, shaving 3/16” from the apex of the COG pathway curve.
4, 5. Knee and ankle motion – The rotation over the calcaneus in early stance with rotation over the metatarsal heads in late stance combined with KF in late stance produces a smooth sinusoidal pathway for the COG.
6. Lateral pelvic displacement – Normal anatomic valgus at the knee and varus at the hip decreases lateral sway, reducing total horizontal excursion from about 6″ to <2″.
MUSCLE ACTIVITY DURING NONDISABLED GAIT
Ankle Dorsiflexors – These muscles (primarily the tibialis anterior, but also the extensor digitorum longus and the extensor hallucis longus) eccentrically contract to smoothly lower the foot from heel strike to foot flat. They also concentrically contract during the swing phase to dorsiflex the ankle and effectively shorten the swinging limb in order to clear the ground.
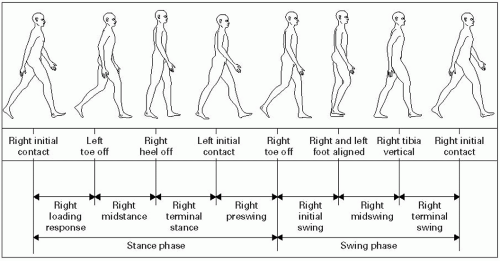 Figure 2-1 Components of the gait cycle. |
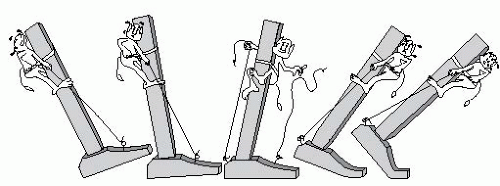 Figure 2-2 The actions of the ankle dorsiflexors/plantar flexors in normal gait. Adapted from Inman V. Human Walking. Philadelphia, PA: Williams & Wilkins; 1981. |
Ankle Plantar Flexors – The triceps surae act eccentrically during midstance to control ankle dorsiflexion caused by the body’s forward momentum. At push-off, they act concentrically to lift the heel and toes off the ground (see Fig. 2-2).
Hip Abductors – The gluteus medius and minimus contract eccentrically during stance phase to limit pelvic tilt of the swing phase leg.
Hip Flexors – The hip flexors (primarily the iliopsoas) contract eccentrically after midstance phase to slow truncal extension caused by the GRF passing behind the hip. The tensor fasciae latae, pectineus, sartorius, and iliopsoas contract concentrically to flex the hip and shorten the limb for effective ground clearance during swing phase.
Hip Extensors – The gluteus maximus and hamstrings start to eccentrically contract just before heel strike to maintain hip stability and slow down the forward momentum of the trunk, since the GRF is anterior to the hip at this stage. They become essentially inactive after foot flat, once the GRF passes posterior to the hip. The hamstrings may weakly contract during the swing phase to flex the knee for ground clearance.
Hamstrings have a double peak of activity just prior to and after heel strike. The first peak occurs during swing phase when there is an open kinetic chain (foot not in contact with ground). This peak decelerates the forward swing of the leg by eccentrically contracting during hip extension and flexing at the knee. At the moment of heel strike, the open kinetic chain is converted to a closed kinetic chain (foot in contact with ground), while the hamstrings act predominantly as a hip extensor preventing both hip and knee buckling.
There is a less consistent peak of activity during late stance phase when hip extension by the gluteus maximus helps propel the COG forward.
Knee Extensors – The quadriceps act primarily to absorb shock during heel strike and keep the knee stable by eccentric contraction. They are also active just before toe-off to help initiate the forward swing of the limb.
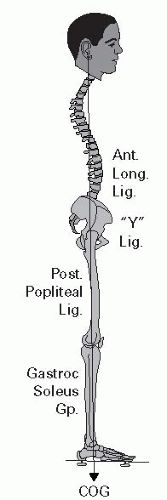 Figure 2-3 The gastroc-soleus complex. Adapted from Cailliet R. Low Back Pain Syndromes. 5th ed. Philadelphia, PA: FA Davis; 1995. |
GAIT DEVIATIONS AND PRESCRIPTIONS
Muscle Deficit Gait
Antalgic Gait – To reduce pain, there is avoidance of WB on the affected limb. The examiner may note a decrease in the stance phase, a reduced step length on the unaffected side, and a prolonged period of double support.
Gastrocnemius Gait – Weak plantar flexors during terminal stance and toe-off prevent adequate heel lift. To limit the drop in the COG that occurs without heel lift during terminal stance, the step length of the contralateral leg is shortened. Treatment: a solid or semisolid AFO with a full-length footplate simulates plantar flexion during terminal stance.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


