Abstract
Objective
Evaluation of the effects of 6 weeks of wheelchair endurance training on arterial stiffness in an individual with paraplegia.
Methods
A 22-year-old male patient with complete (ASIA A) paraplegia (T11) was tested before and after training (30 minutes three times per week). Physical performance and cardiorespiratory response were evaluated during a maximal progressive test. Heart rate (HR), blood pressure, stroke volume and arterial carotid–wrist and carotid–ankle pulse wave velocity (PWV) were measured at rest.
Results
Maximal responses registered (maximal tolerated power, ˙VO2
V ˙ O 2
peak) during the exercise test were increased after training. At rest, HR as PWV decreased, whereas cardiac output and blood pressure remained constant.
Conclusion
Continuous exposure of the subject to a repeated high intensity exercise bout for 6 weeks elevated fitness level. Such a regular practice might also constitute a major way to trigger vascular remodelling beyond to the trained body part.
Résumé
Objectif
Évaluation des effets d’un programme d’entraînement à l’endurance en fauteuil roulant sur la rigidité artérielle d’un sujet blessé médullaire.
Méthodes
Un homme volontaire de 22 ans avec une paraplégie complète (ASIA A ; T11) a suivi un programme d’entraînement en fauteuil roulant (30 minutes trois fois par semaine pendant six semaines). Au début et à l’issu du programme, ses performances physiques et réponses cardiorespiratoires ont été mesurées pendant un test maximal progressif en fauteuil roulant. Sa fréquence cardiaque (FC), sa pression artérielle (PA), son débit cardiaque (Qc) et sa vitesse de propagation de l’onde de pouls (VOP) entre l’artère carotide et l’artère radiale au niveau du poignet et l’artère pédieuse au niveau de la cheville ont été mesurés au repos couché.
Résultats
Les réponses maximales enregistrées pendant l’exercice ont été augmentées après l’entraînement (puissance maximale, pic de consommation d’oxygène). Au repos, FC et VOP ont été diminuées alors que PA et Qc sont restés constants.
Conclusion
L’exposition régulière du sujet à un exercice intense sur une période de six semaines a amélioré son niveau d’aptitude physique. Cette pratique constitue également un moyen de remodelage vasculaire qui s’étend au-delà des territoires entraînés.
1
English version
1.1
Introduction
In individuals with spinal cord injury (SCI), the areas of the body below the level of the lesion are paralysed and therefore extremely inactive, independent of fitness level. As a result, remarkable muscle atrophy can be observed below the level of the lesion. Furthermore, the inactivity and atrophy of the paralyzed muscles lead to a decreased demand for oxygen and, consequently, a decrease in the delivery of oxygen by the circulatory system.
This is observed through vascular adaptations in the legs of individuals with SCI . Detrimental vascular adaptations are related to flow reduction, decreased diameter, decreased arterial compliance of the femoral artery and endothelial dysfunction . Previous research has shown a 40% decrease in diameter and 70% reduction in blood flow through the common femoral artery between trained able bodied subjects and subjects with long-term SCI. It has been demonstrated that the majority of vascular adaptations to inactivity and paralysis is completed within 6 weeks . These peripheral circulatory and skeletal muscle adaptations may contribute to an increased risk of cardiovascular disease in SCI patients.
Regular physical activity may decrease vascular resistance by increasing the number of arterioles and capillaries and the diameter of the conduit arteries. Evidences concerning the vascular bed in the legs of subjects with a complete SCI suggest that endothelial adaptations to exercise training may occur below the level of the lesion. Daily electrically induced training of the legs in subjects with SCI normalized the vascular properties of the femoral arteries . On the other hand, Kingwell et al. demonstrated that 4 weeks of leg training increased the forearm basal production of nitric oxide in the able-bodied subjects. These results suggest that the impact of training on the vascular bed may also involve non-exercised limbs.
In a previous study , we evaluated the effects of an intensive wheelchair exercise training program on able-bodied subjects. The cardiorespiratory response and performance observed during exercise, performed either with arms or legs, were improved after training. According to the known central and peripheral adaptations to arm training , it could be suggested that training provides an important transfer effect in both pairs of limbs.
The systemic adaptations observed in previous studies lead us to raise questions about the effects of an intensive training program performed with the arms, on the vasculature of the paralyzed leg in subjects with SCI.
Based on these previous findings, we applied the same intensive wheelchair training program to a subject with SCI in order to look at the effects on fitness level and arterial stiffness in both trained and untrained limbs.
1.2
Materials and methods
A spinal cord injured male participated in this study (age 22 years, height 175 cm, body mass 65 kg, lesion level T11, ASIA A, time since injury 5 months). His cardiovascular characteristics at rest, physical performance and cardiorespiratory responses recorded during a maximal progressive test were evaluated before and after 6 weeks of interval training.
1.2.1
Evaluation procedure
The subject was tested after a 24-hour abstinence from strenuous exercise, alcohol and caffeinated foods and beverages.
After 30 minutes of rest in the supine position, heart rate (HR) and stroke volume (SV) were measured continuously during 10 minutes, while pulse wave velocity (PWV) and blood pressures (BP) were measured every two minutes. Then, the subject performed a maximal incremental exercise test on a specific wheelchair ergometer.
The progressive wheelchair test started with a resting period of six minutes on the wheelchair ergometer in order to stabilise the different cardiorespiratory variables. This was followed by a two minutes warm up, which was performed at a residual friction power of 15 watts. The load was then stepwisely increased by five watts every two minutes until the subject was no longer able to maintain the required speed. The highest load that could be maintained with a constant speed for one minute was taken as Maximal Tolerated Power (MTP, watts). ˙VO2
V ˙ O 2
peak was determined as the highest ˙VO2
V ˙ O 2
recorded in a 30 seconds average.
Training period: the training procedure has been previously described in 2001 . Briefly, subjects performed 30 minutes of wheelchair ergometry three times per week, for 6 weeks. Sessions consisted of repeated alternating exercise bouts of moderate (four minutes at 50% MTP) and heavy intensity (one minute at 80% MTP). Intensities of both moderate and heavy bouts were selected from the maximal progressive test. The intensity of each training period was adjusted throughout the training program to reach almost 80% of maximal HR by the end of the sixth high intensity interval. When the HR target is not obtained at the end of the session, the training load of the next session is increased by 10 watts.
All training and testing sessions were performed at a cadence freely chosen by the percipient, generally in the range of 1.39 to 1.67 m/s of linear displacement and were performed under medical supervision, with BP control before and after every exercise.
1.2.2
Materials
During the resting period, HR was measured via a wireless Polar-monitoring system (Polar Electro Oy, Kempele, Finland), systolic pressure (SP) and diastolic pressure (DP) were measured using an automatic device (Dynamap ® GE Medical Systems, Buc, France) and SV was measured using an impedance device (Physioflow PF-05, Manatec Biomedical, Paris). The aortic PWV was determined from the foot-to-foot flow wave velocity simultaneously recorded at the right common carotid artery, right brachial artery and dorsalis pedis/tibialis posterior artery using an automatic validated device (Complior SP ® , Artech Medical, Pantin, France). The distance between the site of measurement was estimated according to sex, age, body mass and height of the subjects. A minimum of 10 simultaneously recorded flow waves were recorded and averaged .
During the maximal progressive test, oxygen uptake ( ˙VO2
V ˙ O 2
) and minute ventilation ( ˙VE
V ˙ E
) were continuously determined breath-by-breath during all maximal exercise testing (Cosmed K4 b 2 , Rome, Italy). Gas analysers and turbine were calibrated before each test according to the manufacturer recommendations. HR was continuously measured via a wireless Polar-monitoring system (Polar Electro Oy, Kempele, Finland). For this test and all exercise sessions, the same ergometer (VP100H- HEF tecmachine, Andrezieux Boutheon, France) was used in conjunction with the subject’s personal wheelchair ).
1.2.3
Statistical analysis
All the values are given as the mean (± SD). Training effects on the maximal responses collected during exercise were considered using the delta percent (Δ%) changes calculated from the mean variation ([mean after training − mean before training/mean before training] × 100). Training effects on PWV and BP were analysed considering both delta percent changes and with t-test. Statistical significance was set at the 0.05 level.
1.3
Results
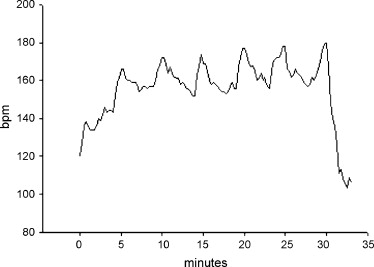
The training program was completed by the subject without excessive fatigue or shoulder pain. The HR monitoring for each training session and the load adjustment on the ergometer enabled the subject to adhere to the intensity recommendations throughout the entire training period. The accuracy of the ergometer in controlling the intensity and duration of exercise may explain the efficiency of our training program. Fig. 1 shows the HR registered during one training session. The HR fluctuations can be observed throughout the exercise and the peak HR obtained at the end of the session (180 bpm).
1.3.1
Effects of training on peak responses during exercise
At the end of each testing session, the subject was exhausted. Peak averages of 30 seconds obtained during maximal incremental tests before and after training are presented in Table 1 .
V ˙ O 2
, ml/min/kg), CO 2 output ( ˙VCO2
V ˙ C O 2
, ml/min), maximal tolerated power (MTP, watts), heart rate (HR, b/min), ventilation ( ˙VE
V ˙ E
, l/min).
| MTP (watts) | ˙VO2 V ˙ O 2 /kg (ml/min/kg) | ˙VCO2 V ˙ C O 2 (ml/min) | RER | ˙VE V ˙ E (l/min) | HR (b/min) | |
|---|---|---|---|---|---|---|
| Before | 40 | 22.7 | 1863.9 | 1.2 | 73.3 | 173.0 |
| After | 50 | 26.36 | 1809.2 | 1.1 | 77.5 | 171.0 |
| % | +25 | +16.1 | −2.9 | −11.65 | +5.8 | −1.1 |
Related posts:
 Dispositif LMD en médecine et métiers de la rééducation : le système européen s’applique en France
Interexaminer agreement of clinical examination of the neck in manual medicine
Sudden dysphagia in an elderly, quadriparetic patient
Dispositif LMD en médecine et métiers de la rééducation : le système européen s’applique en France
Interexaminer agreement of clinical examination of the neck in manual medicine
Sudden dysphagia in an elderly, quadriparetic patient
 Multicenter multidisciplinary training program for chronic low back pain: French experience of the Renodos back pain network (Réseau Nord-Pas-de-Calais du DOS)
Multicenter multidisciplinary training program for chronic low back pain: French experience of the Renodos back pain network (Réseau Nord-Pas-de-Calais du DOS)
 The effect of music therapy on mood and anxiety–depression: An observational study in institutionalised patients with traumatic brain injury
The effect of music therapy on mood and anxiety–depression: An observational study in institutionalised patients with traumatic brain injury
 Return to work of 87 severely impaired low back pain patients two years after a program of intensive functional restoration
Return to work of 87 severely impaired low back pain patients two years after a program of intensive functional restoration
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


