Arthroscopic Treatment of Subscapularis Tears, Including Subcoracoid Impingement
Christopher R. Adams
Patrick J. Denard
Stephen S. Burkhart
DEFINITION
A subscapularis tendon tear typically occurs at its insertion into the lesser tuberosity of the proximal humerus.
Although the subscapularis is the largest of the rotator cuff muscles, historically, it has received little attention.
Subscapularis tendon tears are still often overlooked and underdiagnosed; therefore, a proper evaluation of the shoulder is of paramount importance.
Treatment of subscapularis tendon tears can restore the functional stability of the shoulder.
ANATOMY
The subscapularis muscle originates from the medial two-thirds of the anterior scapular fossa.8 The muscle courses laterally beneath the coracoid and becomes tendinous at the glenoid rim. The subscapularis tendon becomes confluent with the glenohumeral joint capsule deep to it and inserts into the lesser tuberosity of the proximal humerus.
The normal subscapularis tendon not only intermingles with the fibers of the glenohumeral joint capsule deep to it, but at its insertion, it also intermingles with the fibers of the medial sling of the long head of the biceps tendon. The medial sling is composed of fibers from the superior glenohumeral ligament and the coracohumeral ligament complex.
The tendon insertion is about 2.5 cm long (range 1.5 to 3.0 cm) and is trapezoidal, with the widest portion at its most superior (cephalad) aspect (FIG 1).19

FIG 1 • Subscapularis insertion. The subscapularis insertion is wider at its superior aspect and tapers at its most inferior aspect. The insertion resembles the shape of the state of Nevada.
The superior aspect also happens to be the strongest part of the subscapularis insertion.11
The subscapularis muscle is innervated by the upper and lower subscapular nerves, and its blood supply is primarily derived from the subscapular artery.8
The main functions of the subscapularis muscle are to internally rotate and adduct the humerus and to provide an anterior restraint to humeral head translation. The subscapularis also acts in concert with the remaining rotator cuff muscles and deltoid to balance both the coronal- and transverse-plane force couples of the glenohumeral joint.
This results in dynamic stabilization to centralize the humeral head on the glenoid (“maintain the golf ball on the golf tee”), providing a stable fulcrum for glenohumeral motion.
PATHOGENESIS
As with the other rotator cuff tendons, intrinsic factors may play a role in the development of a subscapularis tendon tear. Furthermore, extrinsic mechanical factors have also been implicated in the process.
The normal subcoracoid space (coracohumeral interval) represents the distance from the coracoid tip to the proximal humerus. If this space is stenotic, the coracoid tip will impinge against the insertion of the subscapularis, causing damage to the tendon insertion.
Anatomic and imaging studies have defined the normal coracohumeral interval to be between 8.4 and 11 mm.9,10,15
Subcoracoid stenosis is defined as less than 6 mm of space between the coracoid and the proximal humerus (either by magnetic resonance imaging [MRI] or arthroscopy).15
Patients with subscapularis tears often have a significantly reduced coracohumeral interval (5 mm with subscapularis tears vs. 10 mm without subscapularis tears).17
In subcoracoid impingement, the coracoid abuts against the anterior surface of the subscapularis, causing increased articular (under) surface tensile forces that can cause tendon fiber failure (FIG 2).
Two separate cadaveric studies found that subscapularis tendon tears are often partial-thickness articular tears. Furthermore, they usually begin at the superior aspect of the insertion and are common in the elderly population.20,21
However, complete tears of the subscapularis tendon often result in medial retraction of the tendon edge to the level of the glenoid.
The retracted tendon often pulls with it the adjacent medial sling of the biceps tendon (composed of fibers from the superior glenohumeral ligament and coracohumeral ligament).
The fibers of the medial sling are oriented approximately perpendicular to the fibers of the subscapularis tendon and
arthroscopically appear as a comma-shaped soft tissue structure that we refer to as the comma sign (FIG 3).14
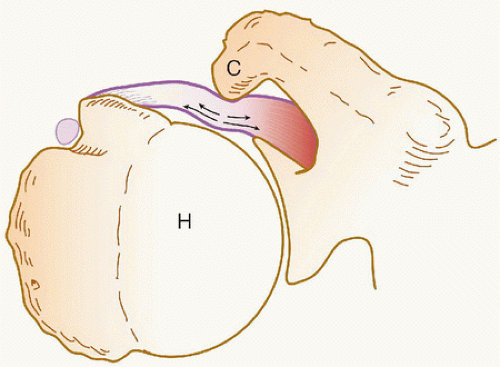
FIG 2 • Schematic drawing of the roller-wringer effect. In patients with subcoracoid impingement, the prominent coracoid tip indents the superficial surface of the subscapularis tendon. This creates tensile forces on the convex, articular surface of the subscapularis tendon, and can lead to failure of the subscapularis fibers. C, coracoid; H, humerus. (From Burkhart SS, Lo IKY, Brady PC. A Cowboy’s Guide to Advanced Shoulder Arthroscopy. Philadelphia: Lippincott Williams & Wilkins, 2006.)
We have found the comma sign to be a useful guide for identifying the retracted superolateral edge of the subscapularis tendon.
The loss of the subscapularis tendon results in an unstable glenohumeral fulcrum and abnormal glenohumeral arthrokinematics.13

FIG 3 • A,B. Anterior structures from a posterior viewing portal of a right shoulder. The medial sling (M) of the biceps tendon (BT) inserts into the lesser tuberosity of the humerus (H) along with the superolateral margin of the subscapularis (SSc). C,D. Complete subscapularis tendon tear. In this situation, the comma sign (,) leads to the superolateral border of the subscapularis tendon. G, glenoid; C, coracoid. (From Burkhart SS, Lo IKY, Brady PC. A Cowboy’s Guide to Advanced Shoulder Arthroscopy. Philadelphia: Lippincott Williams & Wilkins, 2006.)
Chronic tears of the subscapularis should be repaired (even if there is fatty degeneration and significant muscle atrophy) because the subscapularis may have the capacity to function through a tenodesis effect.18
NATURAL HISTORY
There is little available information on the natural history of subscapularis tendon tears.
In some patients (especially those with massive rotator cuff tears), the tears can be disabling. Some patients with massive rotator cuff tears never regain functional overhead use of their arms without surgical intervention.
PATIENT HISTORY AND PHYSICAL FINDINGS
Although most subscapularis tears in the community are degenerative in nature, the classic scenario for a traumatic tear is forced external rotation.2
Forced external rotation results in an eccentric tensile load, which can be particularly dangerous to a “tendon at risk.”
In contrast to patients with the typical posterosuperior rotator cuff tear, who have difficulty with overhead tasks, patients with subscapularis tears often have the burden of diminished function with tasks in front of the body and below the level of the shoulder (eg, opening a jar of food or washing under the contralateral arm).
The typical patient complains of chronic pain and loss of arm strength with activities of daily living in front of the body.
A complete physical examination is necessary, including evaluation of the cervical spine and both upper extremities. Examinations to perform are as follows:
Lift-off test: The test is positive when the patient cannot actively hold the hand away from the lower back; it is positive only when at least 75% of the subscapularis tendon is torn.4 The test is also difficult to perform for some patients with restricted shoulder motion.
Napoleon test, also known as modified belly press: Wrist flexed 90 degrees and elbow posteriorly positioned indicates a positive test; the entire subscapularis tendon is torn. An intermediate test is indicated by wrist flexed 30 to 60 degrees; more than 50% of the subscapularis tendon is torn. A negative test occurs when the patient is able to “strike the pose”; less than 50% of the subscapularis tendon is torn.
With a significant subscapularis tendon tear, the patient flexes the wrist, the elbow drops backward, and the posterior deltoid acts to pull the hand against the belly.
A patient with a subscapularis tear often has diminished internal rotation strength and may have increased passive external rotation (compared to the contralateral extremity) if a complete tear is present.
A patient with a subscapularis tear may also have additional pathology in his or her shoulder.
This again emphasizes the importance of a good physical examination that also evaluates the other rotator cuff tendons, the biceps tendon, glenoid labrum, and so forth.
Patients with a posterosuperior rotator cuff tear often have pain, weakness, and/or limited elevation and external rotation.
A significant tear of the subscapularis tendon may result in disruption of the medial sling of the long head of the biceps tendon. This can lead to either partial or complete tears of the biceps tendon with or without medial subluxation.
A tear of the glenoid labrum often results in “catching” pain that occurs with certain positions of the shoulder, depending on the location of the tear.
IMAGING AND OTHER DIAGNOSTIC STUDIES
We routinely obtain five views of the shoulder: anteroposterior (AP) internal rotation, AP external rotation, AP with 30-degree caudal tilt, outlet view, and axillary plain films.
Evaluation of the plain films may reveal proximal humeral migration (especially with long-standing massive rotator cuff tears), acromial morphology, glenohumeral or acromioclavicular joint degenerative changes, anterior humeral translation (seen with subscapularis tendon disruptions on the axillary view), and so forth.
We also routinely obtain an MRI of the affected shoulder.
The MRI can provide important information on the location and extent of the subscapularis tendon tear.
It can also determine whether additional pathology in the shoulder coexists (eg, additional rotator cuff tears, medial subluxation or tears of the long head of the biceps tendon, ganglion cysts, and labral tears).
Tears of the subscapularis tendon are best appreciated on the axillary and sagittal oblique images of the MRI (FIG 4).1,3

FIG 4 • T2-weighted axial MRI showing a decreased coracohumeral space (yellow line) and complete tear of the subscapularis tendon. Yellow arrow indicates the edge of the retracted subscapularis tendon. (From Burkhart SS, Lo IKY, Brady PC. A Cowboy’s Guide to Advanced Shoulder Arthroscopy. Philadelphia: Lippincott Williams & Wilkins, 2006.)
Signal characteristics consistent with fluid may be seen with partial-thickness tears, whereas a loss of part or all of the normal tendon will be seen with full-thickness tears.
DIFFERENTIAL DIAGNOSIS
Subscapularis tendinitis or bursitis
Posterosuperior rotator cuff tear
Biceps tendinitis
Labral tear
Neurologic impairment
NONOPERATIVE MANAGEMENT
The role of nonoperative treatment in patients with symptomatic subscapularis tears is very limited.
Most patients who present to orthopedic surgeons with subscapularis tears have had the tear for a long time.5
Furthermore, most have attempted and failed nonoperative treatment.
However, for patients who are not good surgical candidates (eg, very old or ill), nonoperative treatment is warranted.
Nonoperative treatment typically consists of activities as tolerated with gentle stretching and progressive strengthening of the shoulder.
SURGICAL MANAGEMENT
Preoperative Planning
The history, physical examination, plain films, and MRI should all be reviewed before operative intervention.
Positioning
The anesthesiologist administers general anesthesia with endotracheal intubation and applies protective eyewear to the patient.
The patient is rotated into the lateral decubitus position and an axillary roll is placed.
The patient is well padded with pillows beneath and between the legs.Related posts:
 Shoulder Arthroscopy: The Basics
Shoulder Arthroscopy: The Basics
 Management of Glenohumeral Instability with Humeral Bone Loss
Management of Glenohumeral Instability with Humeral Bone Loss
 Repair and Reconstruction of Acromioclavicular Injuries
Repair and Reconstruction of Acromioclavicular Injuries
 Snapping Scapula Syndrome
Snapping Scapula Syndrome
 Lateral Epicondylitis (Tennis Elbow) Arthroscopic Treatment
Lateral Epicondylitis (Tennis Elbow) Arthroscopic Treatment
 Open Reduction and Internal Fixation of Fracture-Dislocations of the Elbow with Complex Instability
Open Reduction and Internal Fixation of Fracture-Dislocations of the Elbow with Complex Instability

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


