9
TRAUMATIC KNEE INJURIES
Steven A. Makovitch and Cheri A. Blauwet
OVERVIEW
Traumatic knee injuries are a common occurrence in sports medicine and may greatly impact an athlete’s health and quality of life. With regard to sex-related differences, perhaps no entity has received as much attention as a tear of the anterior cruciate ligament (ACL). Although evidence is less conclusive, other traumatic knee injuries, including meniscal tear, patellar dislocation, and ligamentous injury involving the lateral collateral ligament (LCL) or medial collateral ligament (MCL), may also show sex differences. A thorough understanding of the manner in which these injuries affect male versus female athletes is imperative in the design of patient-specific surveillance, prevention, and treatment strategies.
ANTERIOR CRUCIATE LIGAMENT INJURY
One of the most discussed and studied knee injuries in sports medicine is a rupture of the ACL. The ACL is one of the four main stabilizing ligaments of the knee along with the posterior cruciate ligament (PCL), MCL, and LCL. The ACL extends from the anterior intercondylar region of the tibia to the posteromedial aspect of the lateral femoral condyle and prevents anterior displacement of the tibia (1). The ACL is essential in control of pivoting and cutting movements, and if ruptured, the stability of the knee is compromised (2). Injury to the ACL occurs through two main mechanisms: either by way of contact or noncontact (3,4).
Regardless of how the injury occurs, an ACL tear is a major injury for most athletes. While most athletes returning to cutting and rotational sports choose to undergo surgical reconstruction, recovery usually ranges from 6 to 12 months even if a nonoperative course is pursued (5). An ACL injury also leads to altered biomechanics, muscle weakness, and reduced functional and academic performance, and may lead to the loss of an entire athletic season (6,7). In fact, after an ACL injury only about half of athletes return to a competitive level of sport (8). Additionally, an athlete’s function for many years into the future may also be impacted, as evidence reveals that individuals who tear their ACL have up to an 80% increased risk of developing knee osteoarthritis (OA) 10 to 15 years after injury (6,9–12). From a societal perspective, an ACL rupture is costly, with conservative estimates of surgery and rehabilitation ranging from $17,000 to $25,000 per injury (13,14).
Epidemiology
It has been estimated that 80,000 to 250,000 ACL injuries occur each year in the United States, with more than 50% of injuries occurring in athletes 15 to 25 years of age (15). A study evaluating nationwide incidence of athletes requiring ACL reconstruction found a significant increase between the years 1994 (86,687 injuries or 32.9 injuries per 100,000 person-years) and 2006 (129,836 injuries or 43.5 injuries per 100,000 person-years). This trend disproportionately affected females and those younger than 20 and older than 40 years of age (16).
Significant sex differences exist with regard to the epidemiology of ACL injuries. Female athletes are two to eight times more likely to sustain an ACL injury compared to their male counterparts (16–19). With increasing participation of females in competitive sports, this sex difference takes on even greater importance. Since the enactment of Title IX in 1972, the number of females involved in athletics has grown considerably. The percentage of girls participating in sports at the high school level increased almost 10-fold from 1971 (3.7%) to 1998 (33%). By 1998, females represented 40% of all high school and college athletic participants (20).
The National Collegiate Athletic Association (NCAA) Injury Surveillance System compiled data for eight men’s and eight women’s sports over a 16-year period (1988–2004) from a sample of colleges and universities. In total, the greatest number of injuries occurred in American football. However, if ACL injuries were ranked as a percentage of the total injuries on a team, female sports such as women’s basketball (4.9%), women’s gymnastics (4.9%), women’s lacrosse (4.3%), and women’s soccer (3.7%) showed disproportionate rates of injury. When evaluating the incidence of ACL injury per 1,000 athletic exposures, female gymnastics and men’s spring football showed the highest injury rate (0.33), followed by women’s soccer (0.28) and women’s basketball (0.23) (21,22). Overall, high school athletes show lower rates of ACL injury when compared to collegiate athletes (5.5 versus 15 per 100,000 athlete exposures), however, with a similar distribution of injury across sports (23,24). At the high school level, ACL injuries represent a higher proportion of all injuries in female versus male athletes (4.6% versus 2.5%), with girls’ basketball being the highest (6%), followed by girls’ soccer, girls’ gymnastics, and girls’ volleyball (each 5%) (23). In gender-comparable sports at the professional level, ACL injury rates are similar between sexes (17,22).
The incidence of ACL injury is both sex- and sport-specific. For example, a meta-analysis evaluating sex differences according to sport found a female-to-male ACL tear ratio of 3.5 for basketball and 2.67 for soccer across all age groups and levels. The ratios with lacrosse and alpine skiing were found to be much more equivalent at 1.18 and 1.0, respectively (25). A recent study found that being a college athlete, female, and participating in the sports of soccer or rugby were independent risk factors for having a first-time noncontact ACL injury. After adjustment for sport and level of play, females were more than twice as likely as males to have a first-time ACL injury (relative risk [RR]: 2.10) (26).
Mechanism of Injury
The two main mechanisms of ACL injury are contact and noncontact. Over two thirds of all reported ACL injuries are noncontact in origin, with the remainder originating from contact through an outside force such as another player (3,4). Noncontact ACL injuries typically occur during a deceleration maneuver combined with a change of direction while the foot is in a closed-chain position. When the foot is in a closed-chain position and pronated, the tibia is internally rotated and the knee is at or near full extension (0° to 20° of flexion), the athlete is at particularly high risk. If the athlete attempts to change direction, the result is an excessive torsional force pulling the tibia into internal rotation while the femur is in external rotation, resulting in potential strain or rupture of the ACL (4). Furthermore, the interaction between the trunk and knee is better understood by way of evaluating the hip joint. The kinetic chain directly links the hip to the trunk, which comprises what is known as the lumbopelvic hip complex (27). Hip adduction, internal rotation, and flexion have been described during ACL injury (27–30).
In a study using video analysis to evaluate the biomechanical mechanism of ACL injury during a jumping maneuver, four common motor control strategies were more commonly observed in females. During landing, the injured knee deviated medially, the knee remained in a greater degree of extension, the majority of weight was on a single leg, and the trunk was tilted ipsilaterally. The combination of these components resulted in the center of mass being located outside the base of support during landing, placing the athlete at particularly high risk of ACL injury (29,31). With injury, hip flexion angles have been found to be greater in females compared to males (28,30).
Although noncontact ACL injuries are the most common mechanism of ACL injury, contact injuries can occur, typically via a distinct mechanism. Sports with the highest incidence of contact ACL injuries occur in men’s collegiate American football, ice hockey, and wrestling (22). Soccer has also been found to have a higher percentage of contact injuries than many other sports, accounting for up to 46% of ACL tears (32). The majority of contact ACL injuries in soccer have been found to occur specifically when a player is being tackled (33). Studies from the 1990s showed an incidence of 37% to 48% for contact ACL injuries in soccer (18,32). However, a more recent 2009 study has shown a reduced incidence of 23% (33), possibly due to increasingly strict rules regarding foul play in many contact sports (33).
Due to the preponderance of literature focused on noncontact ACL injury, we focus on this mechanism of injury for the remainder of our discussion. However, it should be noted that the specific definition of “noncontact” ACL injury varies among studies. While some define a noncontact injury as one that occurs in the absence of player-to-player contact, others define it as the absence of a direct blow to the knee (23). Additionally, risk factors for experiencing a noncontact ACL injury can generally be categorized by their ability to be modified (Table 9.1).
TABLE 9.1: Summary of Risk Factors for First-Time Noncontact ACL Injury


Anatomical Risk Factors
There are many proposed anatomical differences between males and females that are important in ACL injury. These sex differences can be divided into primary knee factors and those involving other regions, such as the hip or body mass index (26,34,35). (See Figure 9.1.)
Intercondylar Notch
There has been extensive research evaluating the link between the size and geometric shape of the femoral intercondylar notch and the risk of ACL injury. Two measures of intercondylar notch anatomy include the intercondylar notch width as well as the notch width index (NWI)—that is, the ratio of the width of the anterior outlet of the femoral intercondylar notch divided by the total condylar width at the level of the popliteal groove on a tunnel radiograph (36). Use of this measurement attempts to standardize the notch width relative to overall distal femoral width for individuals of varied body habitus (36). The intercondylar notch has also been classified by geometric shape. An A-shaped notch narrows from the base to the midsection and apex. In U-shaped notches, the midsection does not taper from the base, whereas a W-shaped notch has two apices instead of a classic flat roof (37). There are contradictory findings regarding sex differences in intercondylar notch anatomy. For example, a prospective study of 213 Division I athletes demonstrated that athletes with intercondylar notch stenosis (NWI < 0.2) were at increased risk of noncontact ACL injuries. However, no statistically significant difference was found between the sex of the athlete and notch width indices or rate of ACL tears (38). Another study compared 294 radiographs of athletes both with and without ACL injuries, evaluating notch width and shape. Women were found to have a significantly higher proportion of A-shaped notches when compared to men (34.9% versus 16.7%, respectively), although this was not significantly related to ACL injury given that a smaller notch width and NWI were found in ACL-injured athletes regardless of notch shape or sex (39).

FIGURE 9.1: Sex difference in intrinsic risk factors for ACL tear. (A) Q-angle. (B) Posterior inferior tibial slope. (C) Intercondylar notch width. (D) ACL size.
ACL, anterior cruciate ligament.
Posterior Tibial Slope
An additional anatomical measure called posterior tibial slope (PTS) has been evaluated for its association with ACL injury. PTS is defined as the angle between a line perpendicular to the mid-diaphysis of the tibia and the posterior inclination of the tibial plateau (40). (See Figure 9.1B.) An increase in PTS places the tibia more anterior relative to the femur during quadriceps contraction, which may result in an increased force through the ACL (37). Studies evaluating sex differences with regard to ACL injury and PTS are conflicting, but it seems that there may be an association between PTS and ACL injury, particularly in females. (41–44). A retrospective chart review evaluating radiographs of 199 males and 73 females found that the PTS of the medial plateau was higher in ACL injured females when compared to controls. Additionally, females with ACL injury had a higher PTS than did males with ACL injury (42). Another study used MRI to compare the PTS of those who had experienced a noncontact ACL injury with controls, including both males and females. In the female ACL injured group, the mean tibial posterior slope angle was 10.9° compared to 8.2° in controls (P = .003). Males showed no significant difference between the ACL injured and control groups with regard to PTS (43). Yet another study was done on U.S. Military Academy recruits, in which the PTS was measured on plain film radiographs of 140 individuals with noncontact ACL injuries and compared with controls. Subjects in the noncontact ACL group had significantly greater PTS (P = .003). When broken down by sex, this difference was statistically significant for female subjects (P = .002), however not for males (P = .113) (44). Utilizing MRI, PTS was measured in 100 athletes with a deficient ACL versus 100 control athletes with patellofemoral pain and an intact ACL. An increased PTS was associated with ACL rupture (P < .001) in both males and females; however, there was no statistically significant sex-related difference between groups (41). In sum, emerging evidence points to the contribution of increased PTS as an anatomical risk factor associated with ACL injury in female athletes.
Structure and Function of the ACL
An additional anatomic factor related to sex differences in ACL injury is ligament size. The female ACL has been shown to be inferior in strength and smaller in size than males, which is additionally proven to be unrelated to height (45–48). A cadaveric study found that the ACL in females was smaller in length, cross-sectional area (CSA), volume, and mass when compared to that in males (49). Using MRI in normal individuals, the mid-substance CSA of the ACL was measured. Females were found to have a smaller mid-substance CSA when compared to males even when looking at matched pairs of the same height (P = .008). On average, the CSA was found to be 40% to 50% smaller in females (47). A subsequent cadaveric study evaluating 10 male and 10 female knees revealed that the female ACL may have reduced mechanical strength when compared to the male ACL, even when adjusting for age, body anthropometric measurements, and ACL anthropometric measurements. In this sample, the female ACL was found to fail at 14.3% lower stress when compared to males. The female ACL also had a 22.49% lower modulus of elasticity, meaning that the female ACL offered less resistance during strain (45).
Quadriceps Angle
The quadriceps angle (Q angle) is defined as the angle created between a line drawn from the anterior superior iliac spine to the center of the patella and from the center of the patella to the middle of the anterior tibia1 tuberosity (50). The Q angle has been shown to range from 3.4° to 4.9° greater in females when compared to males and when measured in a standing position (51). Although an increased Q angle in females may lead to more laterally directed pull of the quadriceps at the knee, thus placing the ACL in a position more prone to rupture (20), evidence has not definitively revealed a clear relationship between an increased Q angle and ACL injury (52). A classic study by Shambaugh, Klein, and Herbert evaluated 45 basketball players (sex not specified) and found that the Q angle was higher in those who sustained a knee myotendinous injury or bone contusion compared to those who did not (53). A more recent study from 2004 investigating lower extremity alignment compared 10 male and 10 female subjects with a history of ACL tear with 20 controls. Subjects were assessed on the basis of navicular drop, Q angle, pelvic tilt, hip internal and external rotation range, and true versus apparent leg length discrepancy. Although females had significantly larger Q angles when compared to males, no correlation with ACL injuries was demonstrated. Of these parameters, increased navicular drop and anterior pelvic tilt were found to be statistically significant predictors of ACL injury; however this did not vary by sex (54). There has also been the suggestion that the sex differences in Q angle size can be explained by height, such that taller individuals have smaller Q angles. When males and females of equal height were compared, similar Q angles were found (55). Furthermore, considerable disagreement on the reliability and validity of the clinical Q angle measurement has been noted, possibly due to a lack of standardization (56).
Combination Factors
Combinations of multiple different risk factors for ACL injury have been investigated. A large study involving 895 military cadets found that significant risk factors included a small femoral notch width, generalized joint laxity, and, in women, a higher than normal body mass index (BMI). A combination of these factors greatly increased the risk of injury in females. In females, a multivariate stepwise logistic regression model accounting for narrow femoral notch width, higher-than-average BMI, and generalized joint laxity correctly predicted 75% of noncontact ACL injuries (35). More recently, Sturnick et al. conducted a study to evaluate combinations of intrinsic knee measurements and found these to be more highly associated with risk of experiencing a noncontact ACL injury than individual measurements alone. For example, a smaller femoral intercondylar notch width combined with an increased posterior-inferior slope of the tibial lateral compartment articular surface conferred the greatest risk. Females with both of these variables had double the risk of sustaining an ACL injury. For males, the presence of a smaller ACL volume concomitant with smaller lateral posterior meniscal horn wedge angle increased the risk of ACL injury by 1.76 times (57).
Neuromuscular Control as a Risk Factor
The relationship between neuromuscular control, particularly in movements such as landing and cutting, and ACL injury has been extensively studied (58–60). One reason this area has garnered much interest is that neuromuscular control is considered a modifiable risk factor (34). Additionally, when clinicians and researchers watch athletes sustain a noncontact ACL injury (particularly via video analysis), it appears that there are several common movement patterns that are so prevalent that they are considered “high-risk biomechanical strategies.” Furthermore, these risky patterns are more likely to be displayed by female than male athletes’ positioning (31,61). When evaluated in closer detail, the cumulative forces observed in this landing pattern have been distilled down to four main neuromuscular imbalances that contribute to ACL injury. They are termed ligament dominance, quadriceps dominance, leg dominance, and trunk dominance (29). Each of these is discussed in greater detail in the following sections.
Ligament Dominance
Ligament dominance is characterized by the reliance on bony morphology and static stabilizers such as the ligament to absorb ground reaction force, rather than the larger muscle groups of the lower limb. This results in a high amount of force being translated through the ACL over a very short period of time, which may result in ligament rupture (29). As noted previously, the ACL is the primary static restraint to anterior tibial translation. Through cadaveric testing it has been shown that the greatest forces through the ACL occur with a combination of either (a) anterior tibial shear with internal tibial torque at full extension or hyperextension, or (b) anterior tibial shear with a valgus moment when the knee is at greater than 10° of flexion (62). This corresponds to the aforementioned findings of video analysis of ACL injuries, notably the high-risk position of landing on a straight knee with an accompanying valgus force (29).
Although there have been numerous studies evaluating landing biomechanics in athletes, there is a lack of consistency in the literature regarding typical sex-related differences of knee flexion angles during landing. Although few studies have demonstrated that females land with greater knee extension at initial contact versus males (63,64), most indicate that males and females land with a similar degree of knee flexion (65–68). Similarly, evidence with regard to hip flexion is inconclusive, although most studies reveal no sex differences in the degree of hip flexion during vertical landing tasks (65).
Although most sex-related differences in landing biomechanics lack consistency, one exception is that females have repeatedly been shown to have greater peak knee abduction angles compared to males (66,67,69). It is thought that the peak knee abduction angle in females may represent a lack of ability to control frontal-plane motion of the knee joint, given that females have diminished reflex muscle activation in response to valgus perturbations at the knee (70). This said, video analysis has estimated the time of ACL injury to occur anywhere from 17 to 50 msec after initial contact, while the peak knee abduction angle occurs well past this time period (30,65). Thus, conclusive evidence connecting peak knee abduction angles in females during landing and ACL injury is lacking.
Quadriceps Dominance
Quadriceps dominance refers to the tendency to utilize quadriceps activation to a greater degree than hamstring activation in order to stabilize the knee joint during dynamic movements. Engagement of the quadriceps results in anterior tibial shear force at low knee flexion angles, such as during high-risk landing and pivoting maneuvers, thereby translating a high degree of force through the ACL (29,71). In general, females appear to use the quadriceps to stabilize the knee to a greater degree than males (72). Sex differences have been observed in muscular electromyogram (EMG) firing patterns, with females typically having a higher ratio of quadriceps-to-hamstring recruitment (73,74). For example, one study used an experimental device to translate the tibia anteriorly while asking subjects to resist the force as soon as movement was felt. In these conditions, it was noted that males first activated their hamstrings while females first activated their quadriceps (75). Additionally, findings demonstrate that co-contractions of the hamstring and quadriceps muscles actually decrease the total knee anterior shear force and thus the stress on the ACL (74). If the quadriceps is used primarily for limb stabilization, this only offers a single tendinous insertion for stability and control. Contrast this with the hamstrings that have multiple attachment points, both medially and laterally. The hamstrings can be thought of as a synergist with the ACL because they are able to pull the tibia posteriorly, thus decreasing stress through the ligament (72).
Leg Dominance
In tasks that require symmetry in the lower extremities, females tend to use one leg more dominantly than males. When a female tears her ACL, most of her weight is usually found on a single leg (31). Although most athletes have a preferred plant leg and a preferred kicking leg or jumping leg, the associated asymmetries in muscle strength and recruitment patterns tend to be greater in women than in men (61,69,76,77). Significant differences in knee valgus angles between dominant and nondominant legs have been demonstrated in female high school athletes (69). Another study of female high school athletes revealed significant side-to-side differences in hamstring peak torque and hamstring-to-quadriceps peak torque ratios. It was noted that these side-to-side imbalances were lessened after completing a neuromuscular training program (72). Side-to-side differences in knee abduction angles and knee abduction moments have also shown to be predictive of future ACL tear (58). Leg dominance puts both the dominant and nondominant limbs at increased risk of injury by placing excessive forces on the dominant leg and affording the nondominant limb decreased ability to handle average joint forces (69). Identifying limb asymmetries is therefore an important component of a neuromuscular screening exam.
Trunk Dominance
Trunk dominance is defined as the inability to precisely control the trunk in three-dimensional space (29). Athletes who do not adequately control their trunk have been found to have a greater risk of knee and ACL injury. In a prospective study of athletes, it was found that trunk displacement after a sudden force release was significantly greater (P < .05) in those who went on to have knee, ligament, and ACL injuries. Lateral displacement was the strongest predictor of ligament injury (P = .009). Factors related to core stability predicted risk of athletic knee, ligament, and ACL injuries with high sensitivity and moderate specificity (91% and 68%, P = .001) in female, but not male, athletes (78). Video analysis of ACL injury has also shown a greater mean lateral trunk angle in female compared to male athletes during ACL tear (31). After the pubescent period, females typically experience a shift of weight distribution to their trunk, placing their center of mass further from the ground, although they may not obtain a proportionate increase in neuromuscular development and power unless these factors are specifically addressed in a training program. This excessive trunk motion creates greater torque at the knee joint, further stressing the ACL (58,79).
Dynamic Neuromuscular Control
Although evidence exists in support of each of the four neuromuscular imbalances in relation to ACL injury, limited information is available on the coexistence of multiple biomechanical deficits in the same athlete (Figure 9.2). Biomechanical deficits consistent with ligament and quadriceps dominance have previously been found to coexist in the same group of athletes during drop landing tasks (80). It has also been suggested that athletes who exhibit trunk control deficits in the frontal plane have higher knee valgus moments as the center of mass displaces more laterally (78,81). Recently, the prevalence of biomechanical deficit patterns was quantified in 721 high school female athletes during performance of an unanticipated cutting task. Approximately 40% of females demonstrated no deficits and were categorized as low risk. The next most prevalent profile at 24% was a combination of high quadriceps and leg dominance deficits, labeled as “quadriceps-leg.” This was followed by 22% of females who demonstrated a combination of trunk, leg, and ligament dominance deficits labeled as “trunk-leg-ligament.” The fourth and final profile at 14% demonstrated high ligament dominance deficits only. Further research is needed, but the goal is to better tailor injury prevention programs in relation to an athlete’s specific biomechanical deficit profile (60).
Dynamic control in a jump-landing task has revealed several distinct biomechanical risk factors for ACL injury. Hewett et al. performed a study on 205 female athletes in the high-risk sports of soccer, basketball, and volleyball. Neuromuscular control of the knee joint was prospectively measured using three-dimensional kinematics (joint angles) and kinetics (joint moments) during a jump-landing task. Nine of the athletes went on to sustain an ACL rupture. Comparison of the preseason data demonstrated that ACL injured athletes had knee abduction angles that were 8.4° greater at initial contact and 7.6° greater at maximum displacement during landing. Athletes with ACL injuries had increased angular motion, which took place at a faster pace and with higher forces than in noninjured athletes. Of interest, the authors commented that preseason knee abduction moment measurements could predict which female athletes were at higher risk of ACL injury with a 73% sensitivity and 78% specificity (58). A much simpler instrument, the Landing Error Scoring System (LESS), has recently been examined as a tool for identifying individuals at risk for ACL injury in elite youth soccer. The LESS is a field assessment tool that identifies high risk patterns during a jump-landing maneuver, with higher scores indicating more errors (82). It was found that athletes with a LESS score of five or more were at higher risk. A score of five was optimal as a cutoff point as this produced a sensitivity of 86% and a specificity of 64% as a predictive factor for future noncontact ACL injury (83).
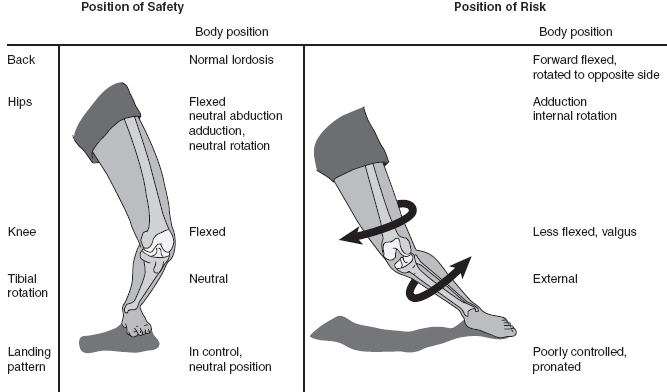
FIGURE 9.2: Knee neuromechanics that have been identified as culprits in anterior cruciate ligament (ACL) injury.
Another recent study evaluated 215 intercollegiate athletes grouped by sex and self-reported history of knee injury. Jump-landing patterns were found to be impacted by sex, but not injury history (84). It was noted that males demonstrated more at-risk landing patterns in the sagittal plane including limited trunk, knee, and hip flexion at initial contact, as well as limited hip flexion throughout the landing. Conversely, females demonstrated more at-risk landing patterns in the frontal plane including knee valgus at initial ground contact and maximum knee flexion, as well as more frontal plane movement throughout the landing (84).
Mechanisms of growth and development in females may underlie the altered neuromuscular control that leads to ACL injury. A study of pubertal males and females was conducted using drop vertical landings. Each subject was evaluated 1 year apart. Interestingly, pubertal females were found to have an increased peak knee abduction angle in the second year when compared to the first year (P < .001), while males showed no change in matched developmental stages (P = .90). It was also found that in postpubertal females, peak knee abduction angle and moment were greater relative to postpubertal males (85).
Fatigue has also been evaluated as a contributing factor to ACL injury. In one study, team sport athletes were compared with dancers during single leg drop landings. Both groups demonstrated suboptimal landing mechanics after a fatiguing protocol, including increased peak knee valgus moment and increased lateral and forward trunk flexion. However, it was noted that dancers took significantly longer to reach fatigue than did the team sport athletes (86). A similar study, again comparing dancers to team sport athletes with single leg drop landings, found female team sport athletes landed with significantly greater peak knee valgus (P = .007) than male team sport athletes and also as compared to both male and female dancers (87). It is hypothesized that slower onset to landing fatigue and better landing mechanics in dancers may be due to the fact that they specifically practice landing technique with high repetitions from a young age. This information may play a future role in preventive strategies.
Sex Hormones as a Risk Factor
Evidence continues to evolve regarding the role of sex hormones in noncontact ACL injury. This body of literature is discussed extensively in Chapter 1 on the influence of sex hormones on the neuromusculoskeletal system.
Genetic Risk Factors
Several studies have suggested that genetic contributions may be considered among intrinsic risk factors for ACL injury. For example, a small study on female twins suggested that neuromuscular imbalance, increased joint laxity, and smaller intercondylar notch width may be associated with ACL injury, each defined as an individual risk factor (as noted previously) but also with a genetic predisposition (88). The background reasons for such familial associations are currently under investigation.
Genetic differences in collagen have also been evaluated as a contributing factor for ACL rupture. A major structural component of ligaments is collagen, predominantly types I and IV, which are encoded by the COL1A1 and COL5A1 genes, respectively. Variations of sequence within these genes may lead to an increased risk of ACL injury (89). For example, a Swedish study found that cruciate ligament injuries were associated with a polymorphism in the COL1A1 gene. Compared with the homozygous ss genotype, the heterozygous participants displayed a similar risk (odds ratio [OR]: 1.06), whereas those with the ss genotype were less likely to experience ACL injury (OR: 0.15) (90). A South African study also revealed that the TT genotype of the COL1A1 Sp1 binding site polymorphism was underrepresented in those with ACL ruptures (91). Another South African study specifically evaluated the COL5A1 gene. It was found that the CC genotype of the COL5A1 BstUI restriction fragment length polymorphism in the female participants was significantly underrepresented in the ACL rupture group compared with controls (27.4% versus 5.6%; OR: 6.6). Male subjects did not reveal a similar correlation (92). Although it is premature to definitively state that genetics play a significant role in the increased risk of ACL rupture in female athletes when compared to males, further study may reveal significant findings in this regard (37).
Injury Prevention
The aforementioned neuromuscular imbalances of ligament dominance, quadriceps dominance, leg dominance, and trunk dominance are each thought to play a role in the underlying modifiable factors contributing to ACL injury. Therefore, many ACL injury prevention programs seek to evaluate for these “high risk” biomechanical strategies in individual athletes during a preseason screening examination, allowing for the implementation of specific neuromuscular training to correct deficits and therefore prevent ACL injury (14,93,94). For example, pre-enrollment drop vertical tests can be administered as a simple, low-cost screen to identify at-risk athletes. Details about the athlete’s knee kinematics can be analyzed (37). In a drop vertical test, the athlete begins by standing on a box (31 cm above ground) with the feet positioned 35 cm apart, then drops directly down off the box and immediately performs a maximum vertical jump, raising both arms as if jumping for a basketball rebound (58). Observations regarding neuromuscular control can include factors such as lower limb alignment, trunk posture, and landing technique, thus helping to focus an individual athlete’s neuromuscular training program. As noted previously in the discussion on neuromuscular control, another simple field assessment screening tool is the LESS, which identifies high-risk patterns during a jump-landing maneuver by simply counting the number of landing “errors” during a jump. Participants jump from a 30-cm-high box to a distance of 50% of their height away from the box, followed immediately by a maximum vertical jump. There are 17 scored items that include assessment of lower extremity, trunk, and foot positioning (82). Good interrater and intrarater reliability can be obtained, and there is concurrent validity using three-dimensional motion analysis (82).
A recent systematic review evaluated the available literature regarding the efficacy of neuromuscular retraining programs in reducing the risk of noncontact ACL injuries. According to the authors, three specific intervention programs were found to be particularly effective: (a) Sportsmetrics, (b) Prevent Injury and Enhance Performance (PEP) program, and (c) the Knee Injury Prevention Program (KIPP). Across these three programs, 70 to 99 athletes needed to be trained in order to prevent one ACL injury, with a relative risk reduction of 75% to 100% (95). Another systematic review evaluated nine ACL injury prevention programs from 1996 to 2008 and found that programs reported a cumulative risk reduction of 52% in females and 85% in male athletes (96).
The Sportsmetrics training program included female high school teams in the sports of soccer, volleyball, and basketball. Participants completed a 6-week preseason neuromuscular training program with a certified athletic trainer and physical therapist involving stretching and plyometric techniques with an emphasis on proper form. Training sessions lasted 60 to 90 minutes, 3 days per week (14). Jump training was based on a prior study that included three phases. The technique phase (Phase I) took place during the first 2 weeks and focused on demonstration and reinforcement of proper jump form. Four basic techniques were emphasized, including maintaining a correct posture (shoulders back, chest over knees, and spine erect), jumping vertically without excessive lean, landing softly with toe-to-heel rocking and bent knees, and lastly, instant recoil preparation for the next jump. The fundamentals phase (Phase II) concentrated on the use of proper technique to build a base of strength and power. The performance phase (Phase III) focused on achieving maximal vertical jump height (72). Throughout the season following Sportsmetrics program implementation, 14 serious injuries occurred in 1,263 athletes, nine of which were noncontact ACL tears. Untrained female athletes were 3.6 times more likely to experience a knee injury than trained female athletes (P = .05) and 4.8 times more likely than trained male athletes (P = .03). The incidence of noncontact knee injuries was significantly lower in the trained versus the untrained female athletes (P = .01) (14).
The PEP program study consisted of female soccer players between the ages of 14 and 18. Each participating team was provided a 20-minute instructional video designed to replace the traditional warm-up performed prior to training and competition. The video consisted of basic warm-up activities, trunk and lower extremity stretching techniques, strengthening exercises, plyometric activities, and soccer-specific agility drills. A heavy emphasis was placed on proper landing technique; for example, maintaining a “soft landing” with deep hip and knee flexion. In the season after program implementation, there was an 88% decrease in ACL injury in the PEP-enrolled subjects compared to an age- and skill-matched control group. In year 2, there was a 74% reduction in ACL tears in the PEP intervention group compared to controls (94).
As another example, the KIPP study evaluated high school female soccer and basketball players and risk of lower extremity injuries. Coaches in the intervention group attended a 2-hour training session 2 weeks before the start of the season, learning how to implement a 20-minute neuromuscular warm-up before team practices and an abbreviated version before games. The warm-up protocol included a combination of progressive strengthening, plyometric, balance, and agility exercises. Athletes were instructed to avoid dynamic knee valgus and to land with flexed hips and knees. After implementation of the program, athletes in the intervention group demonstrated a lower incidence of gradual-onset lower extremity injuries (0.43 versus 1.22, P < .01) and acute-onset noncontact lower extremity injuries (0.71 versus 1.61, P < .01) compared with a control group performing a typical warm-up program. Athletes involved in the program experienced significantly fewer noncontact ACL injuries (Incidence Rate Ratio [IRR]: 0.20; 95% Confidence Interval [CI]: 0.04–0.95). The number needed to treat in order to prevent one noncontact ACL injury was 191 (93).
Soccer is a high-risk sport that has worldwide popularity and is played by almost 300 million people on an amateur or recreational level (97). The FIFA 11+ was developed as a complete warm-up program to prevent injuries in amateur soccer players (98). The program consists of three different components. The first involves running exercises at slow speed combined with active stretching and controlled contacts with a partner. The second component progresses to six different sets of exercises that focus on strength, balance, and jumping. The final component involves speed running combined with soccer-specific movements simulating sudden changes in direction (99). Studies have demonstrated significant benefit of the FIFA 11+ in prevention of ACL injuries in females (100) and in lower extremity injuries in males (101).
Despite these and several other studies demonstrating the benefits of neuromuscular training in the prevention of ACL injuries, the specifics of the composition and duration of the optimal program is still uncertain. A recent systematic review evaluating the ACL neuromuscular training components across 13 studies found that training sessions ranged from 10 to 45 minutes and the total number of sessions ranged from 10 to 108. The emphasis also varied considerably among programs, though most placed the greatest emphasis on balance and agility training (102). It has been suggested that, at a minimum, a prevention program include at least 10 minutes of exercise three times per week with an emphasis on neuromuscular facilitation (96). In 2008, the International Olympic Committee stated that well-designed injury prevention programs should include strength and power exercises, neuromuscular training, plyometric exercises, and agility exercises, along with regular warm-up. The goal of the program should attempt to alter dynamic loading of the tibiofemoral joint through neuromuscular and proprioceptive training and emphasize proper landing and cutting techniques—for example, landing softly on the forefoot and rolling back to the rearfoot, engaging knee and hip flexion, and, where possible, landing on two feet. Training should also avoid excessive dynamic valgus of the knee and focus on the “knee over toe position’’ when cutting (22). Based on prior evidence it is believed that programs should be 8 or more weeks in duration in order to allow sufficient neuromuscular changes and performance training effects (103). Finally, it is important to note that deconditioning after termination of a program can occur quite quickly. Aerobic deconditioning has been reported as soon as 1 to 2 months after program cessation, and anaerobic deconditioning in as little time as 2 weeks, implying that prevention programs should remain ongoing throughout an athlete’s career (15).
Outcomes After ACL Injury
As outlined so far, there is ample evidence to support that female athletes are at higher risk for ACL injury when compared to males. Additionally, females are known to have a greater risk with regard to re-tears of their ACL surgical grafts as well as of the contralateral knee upon return to sport (37). In a study of 1,415 athletes followed prospectively for 5 years after primary ACL reconstruction using a patellar tendon autograft, females experienced more injuries to the contralateral knee when compared to males (7.8% vs. 3.7%; P < .001). There was no sex-related difference in injury incidence to the reconstructed knee (104). Paterno et al. found that almost 30% of young athletes who returned to pivoting and cutting sports after ACL reconstruction suffered a second ACL injury within 24 months after return to sport. Of those who suffered a second injury, contralateral tear occurred 20.5% of the time and ipsilateral graft tear occurred 9.0% of the time. Most injuries occurred early, within 72 athlete exposures. With regard to sex-specific differences, the rate of injury for female athletes in the ACL reconstruction group was almost five times greater (P = .0004) than female controls. Also, a trend was found toward a higher proportion of female participants (23.7%) who suffered a contralateral injury compared with male participants (10.5%), while ipsilateral injuries between males (10.5%) and females (8.5%) were similar. Findings in males were limited due to the small sample size (105). Countering this, a more recent meta-analysis evaluated outcomes of ACL reconstruction, noting no sex-related difference in risk of graft failure or contralateral ACL tear, the latter showing rates of 4% for males and 7.4% for females (P = .13). That said, only a small amount of studies were sufficiently homogeneous to be included in the analysis (106).
With regard to ACL reconstruction, a large epidemiological study evaluated the 3-year cumulative incidence of ACL reconstruction in adult patients. Overall, males were more likely than females to undergo ACL reconstruction after injury (26% versus 19%; P < .001). It should be noted, however, that only adults age 20 and older were included in the study. As one would expect, the likelihood of undergoing ACL reconstruction decreased with each decade of age. For example, 45% of patients age 20 to 29 underwent reconstruction compared with only 8% of patients 60 to 69 years of age (107). Although the majority of orthopedic surgeons recommend ACL reconstruction for those who wish to return to sport (108), not all patients have this goal (109). In fact, a meta-analysis on return to sport after ACL reconstruction found that only 65% returned to their preinjury level of sport and only 55% returned to competitive sport (8). It also demonstrated that males were approximately 1.5 times more likely than females to return to either level of sport (8). Data from the Multicenter Orthopaedic Outcomes Network (MOON) ACL cohort study also found that within the sport of soccer, female athletes are less likely to return to play when compared to their male counterparts (110).
Rupture of the ACL has been found to be a risk factor for future development of knee osteoarthritis (OA). It is commonly stated that, on average, 50% of patients with ACL injury will progress to the development of knee OA later in life (10). With a combined ACL and meniscus injury, this prevalence is even higher (111). The increased risk of OA is most likely related to the extent of the injury to the bone, chondral surface, and meniscus at the time of the ACL tear given that rates of OA are similar regardless of surgical versus nonsurgical management (10,112). A large population-based study in Sweden with a mean follow-up of 9 years found no sex-related difference in the risk of OA after ACL injury (113). Additionally, a systematic review and meta-analysis looking specifically at knee OA after ACL reconstruction concluded the effect of sex could not be determined given that the majority of studies did not publish separate results for males and females (114). Supporting sex-related differences, a 2015 study used MRI to evaluate for the presence of knee OA only 1 year after ACL reconstruction, comparing postoperative subjects with age, sex, and activity-level matched controls. Among those with ACL tear, males were found to have a five to six times greater likelihood of both patellofemoral osteoarthritic changes and the presence of osteophytes (115). Another study from 2014 likewise found sex-related differences with regard to the outcome of progressing to total knee replacement in a 15-year period after cruciate ligament reconstruction. Although the incidence of knee arthroplasty was low at 1.4%, this was seven times greater when compared to a cohort of matched controls. With regard to sex-related differences, being female increased the likelihood of undergoing total knee arthroplasty (hazard ratio [HR]: 1.58; P = .001) (116). More research is needed to determine if a sex-based difference exists with regard to development of OA after ACL injury.
MEDIAL COLLATERAL LIGAMENT/LATERAL COLLATERAL LIGAMENT
Although an abundance of literature exists concerning sex differences in ACL injury, the impact of sex on the knee collateral ligaments is less certain. The two collateral ligaments of the knee, the medial collateral ligament (MCL) and the lateral collateral ligament (LCL), provide medial and lateral stability to the knee joint, respectively. The MCL primarily restricts excessive valgus of the tibiofemoral joint (2). The superficial portion of the MCL is extracapsular while the deep MCL has two attachment points to the medial meniscus (117). The LCL primarily prevents excessive varus of the tibiofemoral joint and has no connection to the meniscus (2).
Overall, the available literature reveals a lack of significant sex-related differences in collateral ligament injury patterns. Two available studies reported the incidence of collateral ligament injuries to be higher in females compared to males, however to a lesser degree than the differences noted with ACL injury. These studies did not differentiate between the lateral versus medial collateral ligaments (17,18). One additional study evaluated the “stiffness” of the medial tibiofemoral joint, comparing sex as well as age in three distinct groups (prepubertal children, postpubertal young adults, and older adults). No sex-related difference was found across the three age groups. However, after puberty, medial tibiofemoral joint stiffness was greater and was significantly influenced by height and mass, regardless of sex (118).
MENISCUS
The knee meniscus is a wedge-shaped section of semilunar cartilage located between the femoral condyle and tibial plateau (119). Both the medial and lateral meniscus play an important role in knee joint stability, shock absorption, as well as nutrition and lubrication of the articular cartilage (120). In one MRI-based study, the cross-sectional shape of the medial meniscus varied significantly between males and females, although much of this was attributable to size-related differences (121). Acute meniscal injuries typically occur when the shear stress generated within the knee during flexion/compression combined with femoral rotation exceeds the meniscal collagen’s ability to resist these forces (2).
Acute meniscal injuries commonly occur in conjunction with ACL tears, and variable sex-related differences with regard to meniscal injury have been reported. A prospective study evaluating meniscal tears during ACL reconstructive surgery found that female high school soccer athletes had fewer medial meniscal tears than did their male counterparts (P = .02), despite finding no sex-related difference in mechanism of injury (122). Another prospective study of 9,023 male and 1,396 female military academy cadets with ACL injury found no significant sex-related difference in the incidence of meniscal injury at arthroscopy (123).
Although less commonly discussed, the incidence of meniscal tear in individuals with intact ligamentous structures has been reported. A case series of meniscal injuries diagnosed at arthroscopy in athletes age 16 to 32 found that males were three times as likely to have the presence of an isolated meniscal tear (120). This finding was similar to that found in a much older review of meniscal injuries (124). A recent study specifically evaluated the prevalence and sex-related variance of isolated meniscal tears in patients younger than 40, revealing that the overall prevalence of meniscal tears was less in females compared with males. In males, the presence of medial meniscal tears increased with age, whereas females revealed a lower prevalence along with no age-related variability. Strikingly, males under 30 were nearly four times as likely to have the presence of an isolated medial meniscal tear compared with females (OR: 3.95 versus 0.25, P = .002) (125). Similar trends have been noted in younger populations. In a study of youth aged 10 to 19 with mixed ligamentous integrity status, complex meniscal tears were more common in male than female children (defined by the presence of open growth plates) (P < .01) (126).
The posterior horn of the medial meniscus is particularly vulnerable to tears as it is relatively immobile compared to other portions of the meniscus. In a single study, radial tears of the medial meniscus posterior horn were uniquely found to be associated with older age and obesity and were more commonly found in females when compared with males (P < .001). In addition, radial tears were strongly associated with an increased incidence and severity of cartilage degeneration compared to horizontal tears (127).
Related to genetic risk factors, molecular analysis of meniscal tissue harvested at the time of arthroscopic meniscectomy has been performed, noting that the expression of the cytokine CCL3L1 was higher in women of all ages with concomitant ACL and meniscal injury. Of note, higher expression of this catabolic marker in patients with a combined injury pattern indicates an increased catabolic response that may lead to greater likelihood of development of post-traumatic osteoarthritis (128).
QUADRICEPS TENDON
Quadriceps tendon ruptures are uncommon and typically occur when the quadriceps muscle rapidly and eccentrically contracts with the knee in a semi-flexed position (129). Males have been reported to incur this injury four to eight times more often than females (129–132), potentially due to the disproportionately increased prevalence of systemic risk factors such as gout, metabolic disease, and chronic renal failure within the male population (133,134). Rupture typically occurs in the sixth decade of life (129,132,135). The most commonly reported scenarios of injury occur with a simple fall (61.5%) or a fall from stairs (23.4%). Injury during an actual sporting activity is reported to be far more rare (6%) (135). Treatment typically involves surgical repair, for which one study revealed no sex differences in outcomes (136).
PATELLAR DISLOCATION
An acute traumatic patellar dislocation usually occurs in young, active individuals (137–139). The typical mechanism of injury underlying acute patellar dislocation is partial flexion of the knee with tibial valgus (139). Athletes displaying an increased Q angle at 30° of flexion may be at higher risk (140), and one cadaveric study revealed that relaxation of the vastus medialis oblique (VMO) also reduced lateral stability (144). A similar incidence of injury between males and females has been reported (137,141). However, when evaluating young, active individuals, there is a definite female predisposition toward injury that lessens with age (137–139,142). A prospective, population-based study found that the risk of first-time patellar dislocation is 33% higher among females than males when examining individuals age 10 to 17, which is a high-risk age group. The risk of patellar dislocation was three times higher in females with a prior history of either dislocation or subluxation (138).
Knowledge regarding specific characteristics of anatomical risk factors between males and females is limited. Anatomic differences in females have been found to include joint hypermobility, increased femoral torsion, and extensor mechanism malalignment (138). One study specifically used MRI to evaluate for anatomical sex differences in those who sustained a patellar dislocation, comparing these with a control group. Trochlear asymmetry was higher in females, whereas trochlear depth was higher in males (143). This bears importance given prior studies demonstrating that a flattened trochlear groove reduced lateral knee stability by 70% at 30° of flexion (144). A significant interaction between patellar dislocation and sex was also observed for the tibial tubercle–trochlear groove (TT-TG) distance (P = .02), which was longer in females and also correlated with an increased Q angle (145). In this particular study group, injury during low-risk and no-risk pivoting injuries were more common in females, whereas first time dislocations in males occurred predominantly during high-risk pivoting activities (143).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


