CHAPTER 24 Neuromuscular Scoliosis
General Principles
Natural History and Associated Complications
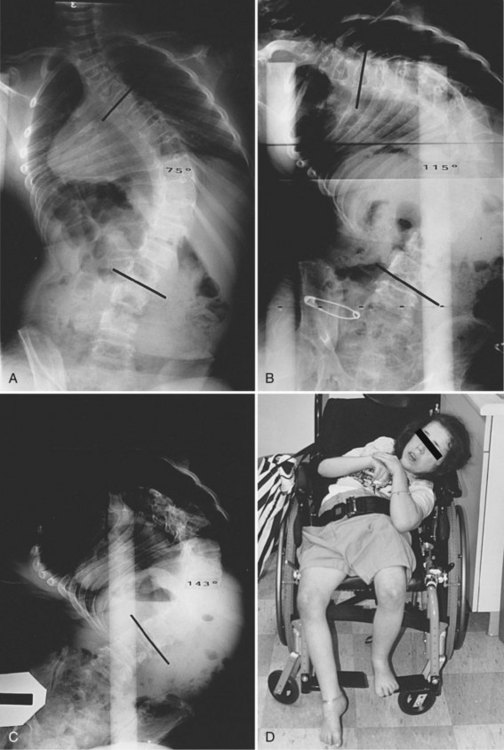
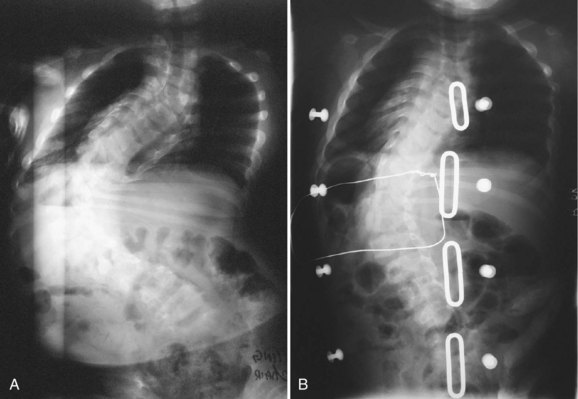
Neuromuscular scoliosis generally begins early in life, is rapidly progressive, and causes significant morbidity. Some patients are capable of ambulation, although many lose their ability to walk early in life or never achieve ambulatory status at all. The use of a wheelchair affords these patients educational and social opportunities that enrich their lives. Spinal deformity can impair comfortable sitting and dramatically reduce the individual’s quality of life. Unbalanced curves and significant pelvic obliquity make wheelchair positioning difficult and may cause uneven distribution of weight that may lead to pressure sores (Fig. 24–1). Prominences created by the convexity of a curve may result in skin breakdown; creases within the concavity of the trunk deformity are susceptible to skin maceration and infection (Fig. 24–2). Majd and colleagues1 showed a correlation between deformity size, functional decline, and decubitus. Large rigid curves restrict lung volume and impair respiration in patients who often already have limited pulmonary capacity. Treatment of neuromuscular scoliosis can also help the caretakers of these patients, improving the ease of transfers, positioning, feeding, and hygiene. The ultimate goal of treatment of patients with neuromuscular scoliosis is the maintenance of as much independence and function as possible. When patients with neuromuscular scoliosis lose the ability to sit comfortably, their quality of life is dramatically decreased. The natural history for a given patient is largely determined by the specific underlying neuromuscular condition and the degree of involvement.

Nonoperative Treatment
Medical Treatment
Spinal Muscle Atrophy
Various medications have been tested to improve the musculoskeletal function of patients with neuromuscular disorders. Randomized placebo-controlled trials have been conducted investigating the efficacy of several medical treatments for SMA, including creatine, phenylbutyrate, gabapentin, and thyrotropin-releasing hormone.2–5 None of these compounds has proven to be an efficacious drug treatment for SMA.2
Cerebral Palsy
Several medical therapies have been investigated for the treatment of spasticity in patients with cerebral palsy. Botulinum toxin has gained a growing acceptance as a treatment of upper and lower limb spasticity. Initial reviews of the literature by the Cochrane Collaboration and others yielded inconclusive evidence that could neither confirm nor deny the efficacy of botulinum toxin in the treatment of spasticity.6 Inclusion of more recent randomized controlled trials into the analysis has provided evidence that supports the use of botulinum toxin to provide a time-limited benefit to decrease muscle tone in children with upper and lower limb spasticity associated with cerebral palsy.7 Although evidence for the use of botulinum toxin is not yet conclusive, the evidence trend is in favor of using this therapy to reduce spasticity associated with cerebral palsy.
Intrathecal baclofen is a well-established treatment that has been shown to provide significant benefits in controlling spasticity in patients with cerebral palsy. Intrathecal baclofen has been shown to reduce the need for orthopaedic lower extremity procedures and the rate of postoperative complications associated with these procedures.8 Concerns have been raised, however, regarding its impact on the progression of scoliosis in patients with spastic quadriplegia. In a retrospective review, Ginsburg and Lauder9 found a sixfold increase in the rate of scoliosis curve progression at 2-year follow-up in a group of 19 spastic quadriplegic cerebral palsy patients. Caird and colleagues10 showed a significantly higher rate of complications associated with posterior spinal fusion and instrumentation in a group of 20 spastic cerebral palsy patients with intrathecal baclofen pumps compared with a matched control group. This study was limited by its relatively small sample size and lack of a control group. Shilt and colleagues11 found no difference in curve progression at 3-year follow-up between 50 cerebral palsy patients treated with intrathecal baclofen and 50 matched control cerebral palsy patients. Based on the current evidence, no significant conclusions can be drawn about the impact of intrathecal baclofen pumps on the progression or treatment of spinal deformity in patients with cerebral palsy. Baclofen can provide significant relief of spasticity, and this evidence must be considered in the context of any potential side effects.
Duchenne Muscular Dystrophy
Advances in general care, glucocorticoid treatment, noninvasive ventilatory support, cardiomyopathy management, and scoliosis management have significantly changed the course of Duchenne muscular dystrophy (DMD). Survival into adulthood is now a realistic possibility for many patients who received optimal treatment.12 Although gene-based and cellular-based therapies are currently under development for the treatment of DMD, the efficacy of glucocorticoid steroids has been evaluated by several randomized controlled trials. In their Cochrane review and meta-analysis, Manzur and colleagues13 concluded there is evidence that muscle function and strength are improved in the short-term (6 months to 2 years) with corticosteroid therapy. The authors based their conclusion on six randomized controlled trials and observed that the most effective prednisolone dose seemed to be 0.75 mg/kg/day, given daily.13 Markham and colleagues14 showed that glucocorticoid therapy provides the added benefit of retarding the anticipated development of ventricular dysfunction if begun before ventricular dysfunction in their series of 14 DMD patients treated with steroids compared with 23 DMD patients treated without steroids.
Genetic and Family Counseling
Because of the complexity of the medical and psychosocial issues associated with neuromuscular disorders and spinal deformity, care needs to be coordinated with a multidisciplinary team. The primary care physician should be well informed of all orthopaedic issues and play a central role in managing care. Psychosocial support for patients and parents is also vital. Patient advocacy groups have proved to be very useful in helping families cope with the illness and associated surgical care. Physicians may wish to provide information regarding clinical trials or refer families to clinical trial websites (www.clinicaltrials.gov provides a current listing of open clinical trials). Patients and parents may need to be referred for genetic counseling to confirm the patient’s diagnosis and aid in family planning.
Bracing
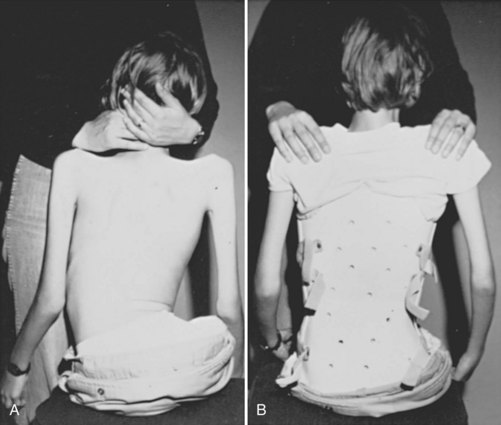
Bracing is a controversial treatment method in idiopathic and neuromuscular scoliosis. Bracing in neuromuscular scoliosis may be used for postural support, although there is incomplete evidence of its efficacy in limiting curve progression (Fig. 24–3). The etiology of the patient’s scoliosis and the patient’s muscle tone have an impact on the practicality of brace treatment. Patients with spastic disorders generally do not tolerate rigid brace treatment, whereas patients with flaccid paresis are more apt to be compliant with brace treatment. The type of orthoses may play a role in the outcome of the treatment.
Kotwicki and colleagues15 followed 45 nonambulatory patients with neuromuscular scoliosis treated with a suspension trunk orthosis (STO) and found that the STO slowed curve progression in 23 patients. The STO construction functions contrary to the classic thoracolumbosacral orthosis (TLSO), with the STO not resting against the patient’s pelvis but rather directly against the seat. The evidence supporting STO use to prevent curve progression is limited, however, and skin intolerance found in 36 patients complicates its clinical practicality. Although there is limited research on the results of the STO brace, there are numerous studies investigating the TLSO brace. In a study of 15 patients, Shoham and colleagues16 found that a TLSO reduced scoliotic deformity and pelvic obliquity leading to reduced sitting pressure. These results are contrary to other studies reported in the literature. In a study of 23 patients, Miller and colleagues17 followed 23 patients with cerebral palsy who wore a rigid Wilmington TLSO for an average of 67 months and concluded that the bracing did not slow progression of their deformity. Olafsson and colleagues18 followed 90 patients with various neuromuscular conditions treated with a soft Boston orthosis for an average of 3 years after brace treatment. They concluded that brace wear was indicated only in a limited subset of patients—ambulatory patients with hypotonia and short thoracolumbar curves (<40 degrees). In all other patients, brace wear was ineffectual in altering progression but did provide assistance in sitting.
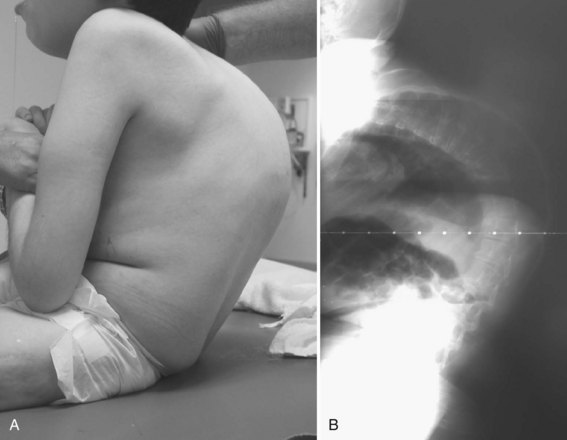
Patients with neuromuscular scoliosis may lack sensate skin to feel pressure from the brace or the muscular control to pull away from the sides of the brace. These patients rarely tolerate the rigid braces often used in idiopathic scoliosis. Patients tend to tolerate soft TLSOs designed to provide improved sitting stability and head and trunk control, while limiting discomfort and skin breakdown (Fig. 24–4).19
The impact of the orthosis on pulmonary function is another important factor to consider when contemplating a TLSO for patients with neuromuscular scoliosis. The effect of bracing on pulmonary dysfunction seems to depend on the level of muscle spasticity. Flaccid patients are more amenable to rigid bracing, although this bracing may significantly decrease chest expansion leading to compromised pulmonary function.20 Spastic patients seem to be more amenable to soft bracing, which does not seem to compromise pulmonary function,21 although this bracing has been shown only to enhance seating comfort.17 Olafsson and colleagues18 and Bunnell and MacEwen22 suggested that a subset of patients with minimum deformity and muscle hypotonia or mild spasticity may experience slowing of curve progression by bracing without a negative impact on pulmonary function.
Other factors to evaluate when choosing orthotic treatment for neuromuscular scoliosis include ease of application and obstructions. A bivalved brace may be easier for a caregiver to place, although it cannot provide as much corrective strength as a single opening brace. Winter and Carlson23 found the two-piece bivalved brace to be a useful support in children with myelomeningocele and SMA. Patients with a stoma or gastrostomy tube require modification of the brace to accommodate these features.
If a patient is not a candidate for bracing or surgery, wheelchair modifications can aid in providing a more comfortable seating position. Modular seating systems can be configured for optimal support of an individual patient (Fig. 24–5). A biomechanical evaluation of seating insert configurations by Holmes and colleagues24 concluded that three-point force application provides significant sitting support and static correction of scoliosis. Patients with more severe deformity may benefit from custom-molded seatbacks, although these items are expensive, and younger patients may outgrow them quickly.

Operative Treatment
The timing for operative treatment is influenced by curve severity, underlying neuromuscular pathology, and other factors. The curve severity guidelines are loosely based on, but less aggressive than, the guidelines used in idiopathic scoliosis. Fusion should be considered as coronal deformity approaches 40 to 60 degrees. DMD may be an important exception to this concept: Surgery has been advocated when the deformity reaches 20 degrees because of pulmonary considerations.25 Patients with severely limited respiratory function have been shown to have good outcomes in spinal surgery, however. The sagittal profile is another important consideration because lordotic and kyphotic deformities can also impair sitting balance and pulmonary capacity (Fig. 24–6). Other factors that play a role in the decision to operate include patient age, nutritional status, cardiac function, curve progression, patient comorbidities, and family and caretaker support.
The benefit of scoliosis surgery in this population is a topic of much debate. Many of these patients are poor operative candidates and risk much undergoing involved corrective surgery. Preoperatively, patients may have compromised pulmonary function, limited cardiac capacity, poor bone stock, and high risk for aspiration, which put them in danger of intraoperative or postoperative complications. Correction of large deformities requires extensive exposures and long procedures that can lead to blood loss greater than one to two patient blood volumes. Although many patients already have neurologic compromise, they are still at risk for further compromise because of intraoperative spinal column manipulation. More powerful instrumentation systems have led to less postoperative decompensation and pseudarthrosis; however, there remains a considerable risk of curve progression, sometimes necessitating revision surgery.26–28
Despite the risk of surgery, the benefits of corrective scoliosis surgery for many of these patients are substantial. Halting or slowing curve progression has a positive impact on the functional ability, comfort, and overall quality of life of these patients. Lonstein and Akbarnia29 reported that more than 50% of patients treated had functional improvement after surgery. In a study of 79 patients with total body spastic cerebral palsy, Comstock and colleagues27 found that 85% of caretakers surveyed were satisfied with the surgery, reporting improved comfort, sitting ability, and cosmesis for the patients. Bridwell and colleagues26 found similar trends in a study of 54 patients with neuromuscular disorders with all caretakers reporting benefit from the surgery, specifically in the areas of ease of patient care, skin breakdown, patient comfort, pulmonary complications, and quality of life. Askin and colleagues30 evaluated 20 patients with neuromuscular scoliosis preoperatively and 6, 12, and 24 months after corrective spinal surgery. The authors noted decreased physical ability at the 6-month time point followed by a return to preoperative function by 12 months and concluded that scoliosis surgery in these patients can stabilize, but not improve, function; however, 75% of patients or caregivers were extremely pleased with the cosmetic results of the surgery. Although most of these patients have deteriorating courses, the correction of spinal deformity seems to improve their function and quality of life.
Although these positive results make a strong case for spine surgery in patients with neuromuscular scoliosis, several review studies have been unable to show a clear benefit of surgical intervention for the patient. Mercado and colleagues31 evaluated 198 publications and graded their results on the concept of Grades of Recommendation introduced in the Journal of Bone and Joint Surgery.32 These authors concluded that the current literature shows there is poor-quality evidence that spinal fusion improves the quality of life in patients with cerebral palsy or DMD.31 In a Cochrane Collaboration review, Cheuk and colleagues33 found that there were no randomized controlled clinical trials available to evaluate the effectiveness of scoliosis surgery in patients with DMD, and so no evidence-based recommendations could be made. Although the practicality of conducting a randomized controlled trial of this nature is questionable, the literature does not provide sufficient evidence to support the role of spinal surgical treatment in patients with neuromuscular scoliosis. It is recommended that the decision for surgical intervention be made based on the needs of the individual patient in consultation with the multidisciplinary neuromuscular care team.
Preoperative Considerations
Neurologic
Many patients with neuromuscular scoliosis are on long-term seizure therapy, which has some important operative ramifications. Antiepileptic medications such as phenytoin and valproate have been linked to decreased bone turnover and decreased intestinal absorption of calcium resulting in osteopenia, which may affect implant fixation and should be considered in the selection of construct components.34,35 In addition, valproate is associated with decreased von Willebrand factor and an increased bleeding time. If possible, consideration should be given to weaning the patient off of this medication, or at least the surgeon should prepare for increased blood loss by having supplementary blood products available during surgery. Preoperative screening of complete blood count, prothrombin time, and partial thromboplastin time may not be predictive of intraoperative coagulopathy.36
Pulmonary
Full pulmonary assessment should be conducted by a pulmonologist and include a chest radiograph, arterial blood gases, and pulmonary function tests if the patient’s developmental age is at least 4 years old. Vital capacity that exceeds 500 mL and peak expiratory flow greater than 180 mL/min are associated with decreased perioperative pulmonary complications. Although surgery may be considered in appropriately selected patients with preexisting respiratory failure, Gill and colleagues37 showed that patients with a forced vital capacity (FVC) of 20% of predicted value can safely be operated on for deformity correction. This prospective observational study followed eight patients on noninvasive night ventilation for respiratory failure with 48 months after surgery and found that all patients recovered well with no major complications. If a patient cannot be assessed with formal pulmonary function tests, other signs of ventilatory capacity must be used, including crying, laughing, and other vocalizations.38–40
Nutritional
Proper nutritional balance is crucial for successful surgical outcomes in patients with neuromuscular scoliosis. Many patients are malnourished secondary to a combination of reflux, low calorie intake, and high metabolic demand from frequent illness. Malnourished patients are more prone to perioperative complications such as wound dehiscence, wound infection, and pulmonary complications. Conversely, older patients may be obese, presenting further operative complications associated with their body habitus. Nutritional status should be assessed preoperatively with albumin and total blood lymphocyte levels. Albumin should be greater than 3.5 g/L, and total lymphocyte count should be greater than 1.5 g/L40; in a study of 44 patients, Jevsevar and Karlin41 found that patients had a lower incidence of postoperative infections if they met these criteria.
Cardiovascular
Patients may have cardiac problems secondary to their deformity and other cardiac issues that are comorbidities of the primary disorder. Thoracic cage deformity resulting from scoliosis can cause hypoventilation and subsequent increased pulmonary vascular resistance; this increased vascular resistance can cause right ventricular hypertrophy and eventually cor pulmonale. Patients with DMD may have cardiomyopathy and arrhythmias. The complications associated with arrhythmias may be alleviated with glucocorticoid steroid treatment.14 Patients with myotonic dystrophy may also have cardiac arrhythmias. Left ventricular hypertrophy can be associated with Friedreich ataxia.
Hematologic
Studies have shown that patients with neuromuscular scoliosis have greater blood loss than patients with idiopathic scoliosis undergoing similar procedures. In this neuromuscular group, the underlying disorder plays a major role in determining the extent of blood loss. In a review article, Shapiro and Sethna42 found that patients with DMD had the greatest mean levels of blood loss. Much of this difference is due to the requirement for larger fusions in patients with neuromuscular scoliosis, although osteopenia in these patients may also play a role.43,44 Preparation for major blood loss—sometimes exceeding 200% of a patient’s blood volume—is essential.38 Often, these patients have already had major surgery, and previous blood loss experience can be used as a guideline for preoperative preparation. Patients should have partial thromboplastin time, prothrombin time, and platelet function evaluated as a part of their preoperative blood work; a more aggressive coagulopathy workup should be conducted if the patient has previously shown a tendency toward excessive blood loss.
In a prospective, double-blinded, placebo control study of 40 pediatric patients, Neilipovitz and colleagues45 found that tranexamic acid administration significantly reduced perioperative blood transfusions. These results have been supported by a meta-analysis by Gill and colleagues,46 which found that tranexamic acid and aminocaproic acid are effective in minimizing blood loss and transfusion in patients undergoing spine surgery. The side effects for tranexamic acid and aminocaproic acid are minor but should be discussed with the patient before using these agents. The surgeon and the anesthesiologist should familiarize themselves with these agents and make a collaborative decision on their use based on the needs and concerns of the individual patient.
Radiographic Assessment
Patients should have a preoperative anteroposterior and lateral film taken of the entire spine preferably in an upright (sitting or standing) position. For assessment of skeletal maturity, a separate anteroposterior radiograph of the pelvis should be considered because scoliosis films often truncate the anatomy necessary to determine skeletal maturity. To assess spinal flexibility, supine bending films or traction films are used. Accurate measurements of the coronal Cobb angle, sagittal Cobb angle, and pelvic obliquity are crucial for complete preoperative planning and postoperative evaluations. In a more recent analysis of the interobserver and intraobserver variability of radiographic measurements of patients with neuromuscular scoliosis, Gupta and colleagues53 found that neuromuscular radiographs can be reliably analyzed with the use of coronal Cobb angle. Patients who may have congenital spinal anomalies or spinal tethering, such as patients with myelomeningocele, should undergo magnetic resonance imaging (MRI) to evaluate the neural elements fully before surgery. Computed tomography (CT) may also be useful in some patients with severe deformity or in patients with a congenital malformation of the vertebrae.
History of Instrumentation in Neuromuscular Scoliosis
In 1942, Haas47 published one of the first references to surgical intervention in neuromuscular scoliosis: a case report describing muscle and fascial transfers to obtain complete and permanent correction in one patient. With the introduction of the Harrington rod in 1962, use of this instrumentation with fusion of the spine in patients with neuromuscular scoliosis became the standard. Series using only Harrington rods and posterior spinal fusion have been associated with high incidences of pseudarthrosis (19% to 40%), moderate initial correction (20% to 57%), and loss of correction ranging from 14% to 28%.29,48 After Harrington rod instrumentation, most patients required bed rest and bracing or casting for up to 1 year.
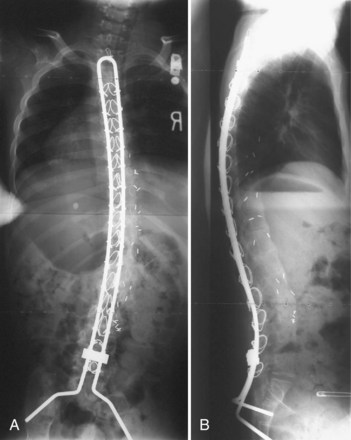
The introduction of segmental spinal instrumentation by Luque49 in 1976 led to major advances in the biomechanical stability and correction of these very deformed spines (Fig. 24–7). Several studies revealed that Luque segmental sublaminar wire fixation had fewer complications than Harrington instrumentation and was stable enough so that most patients required no brace or cast postoperatively.48,50,51 Using the Luque method, the only patients with cerebral palsy requiring postoperative bracing may be patients with athetosis or poor fixation because of severe osteopenia. This is a tremendous advantage because postoperative casting carries the potential for skin and pulmonary complications. Because of these attributes, the Luque technique became the standard method for posterior spinal instrumentation in patients with neuromuscular spinal deformities.

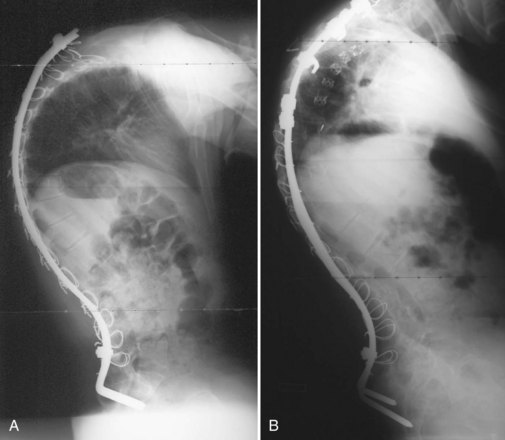
Contouring Luque spinal rods after the technique introduced by Allen and Ferguson52 (Galveston technique) allowed the rods to be fixed to the pelvis, providing surgeons with a more effective method of controlling pelvic obliquity. Bell, Moseley, and Koreska developed the unit rod, a precontoured U-shaped rod that includes the Galveston portion for pelvic fixation (Fig. 24–8). Studies of patient outcomes with unit rod fixation have revealed excellent correction and maintenance of correction.54–56 Bulman and colleagues57 compared the unit rod with double Luque rods and reported superior correction of sagittal and coronal alignment and pelvic obliquity with the unit rod constructs. Tsirikos and colleagues56 evaluated 287 children treated with unit rod instrumentation to the pelvis with 2-year follow-up and concluded that it offers the advantages of good correction of deformity and pelvic obliquity, a low complication rate, and a 96% caretakers’ survey satisfaction rate. Unit rod instrumentation has also been shown to have good results in ambulatory patients, with excellent deformity correction and preservation of ambulatory function at 2.9-year follow-up in 24 patients.58 Additionally, biomechanical studies have shown that the addition of an L5 pedicle screw increases the construct stiffness and the strength-reducing complications associated with the loss of fixation.59
Through a desire to achieve similar correction as the unit rod construct, without the need for pelvic fixation, the U-rod was investigated by McCall and Hayes.60 This rod is an outgrowth of the unit rod concept except the rod terminates in pedicle screws at the L5 level relying on the iliolumbar ligaments to achieve correction of the pelvic obliquity. In their comparison study of 30 patients with unit rod instrumentation and sacral fusion and 25 patients with U-rod instrumentation and L5 fusion, McCall and Hayes60 found that the U-rod provided comparable correction of scoliosis and pelvic obliquity in curves with less than 15 degrees L5 tilt at 4 years of follow-up. Regardless of whether the precontoured unit rod or double Luque rods are used, segmental sublaminar wire instrumentation provides simple, inexpensive, and fairly powerful correction of coronal plane deformity. Segmental sublaminar wire instrumentation has limitations in the maintenance of sagittal plane alignment, however, because the sublaminar wiring fails to fix spinal length, and the vertebrae can slide along the smooth rod construct, particularly during trunk flexion (Fig. 24–9A).
Multihook segmental systems such as Cotrel-Dubousset (CD) and Isola have also been shown to be efficacious in patients with neuromuscular scoliosis.61–63 The comparative efficacy of these two different constructs is inconclusive. In a study of 47 patients with neuromuscular scoliosis, Yazici and colleagues64 concluded that the Isola instrumentation combined with Galveston pelvic fixation provided correction and maintenance of pelvic obliquity superior to Luque Galveston, unit rod, or CD instrumentation. The results of this study are in contrast to the work of Wimmer and colleagues,63 who found that there was no difference between Luque Galveston and Isola instrumentation in radiographic outcomes, patient satisfaction, or complication rate. The selection of either of these two instrumentation systems is a choice that relies on surgeon experience and the needs of the individual patient.
Pelvic and Sacral Fixation
Severe pelvic obliquity secondary to unbalanced scoliotic curves and lower extremity contractures is common and progressive in patients with neuromuscular scoliosis. A solid spinal fusion to the pelvis aids in sitting comfort and balance1,65; however, achieving this goal can be troublesome (Fig. 24–9B). Controlling the motion across the lumbosacral joint requires secure fixation to the pelvis to prevent a pseudarthrosis.
Various systems have been proposed to provide fixation to the pelvis. The Galveston technique was the first advancement to improve fusion rates and clinical success in long fusions to the sacrum.52,53 When paired with either contoured Luque rods or unit rods, it provides powerful coronal correction of pelvic obliquity. This technique places greater forces, however, on the lumbrosacral junction, and proper contouring of the rods may be difficult. The initial concern regarding the association between radiolucency around the screw tips (“windshield wiper” sign) and an increased incidence of complications is of little clinical significance (Fig. 24–10).66,67 Although a biomechanical evaluation of the Galveston technique by Sink and colleagues28 showed that this construct creates a long lever arm that places considerable cantilever forces at the lumbrosacral junction, these forces lead to a high incidence of proximal fixation pullout and distal migration of Galveston rods. The rods also require three-dimensional bending that makes it difficult to contour the rod properly.68

Other systems of sacropelvic fixation use an “S” bend (Dunn-McCarthy), which hooks distally over the sacral alae, while the more proximal portion is secured to the lumbar spine at L4 or above with a pedicle screw or infralaminar hook. Reviewing the results of 67 patients, McCarthy and colleagues69 found that this technique had decreased operative time compared with Galveston fixation and excellent clinical results, although in 2 of the 67 constructs there was migration of the rods into the pelvis. Other techniques of rod contouring to fix to the pelvis include the Warner-Fackler and McCall techniques, both commonly used in the treatment of myelomeningocele-associated kyphosis in which posterior elements of the lumbar or sacral spine may be absent. In the Warner-Fackler technique,70 Luque rods are bent to 90 degrees in two places at the distal end, allowing the rods to pass through the S1 foramina and lever against the front of the sacrum to provide sagittal correction (Fig. 24–11). In a slight variation of this technique, McCall71 described bending Luque rods to 20 to 40 degrees, passing them through the S1 foramina and bending the protruding portion according to the contour of the anterior sacrum. In 16 myelomeningocele patients with hyperkyphosis, McCall71 found satisfactory correction and maintenance of correction after 5 years of follow-up.
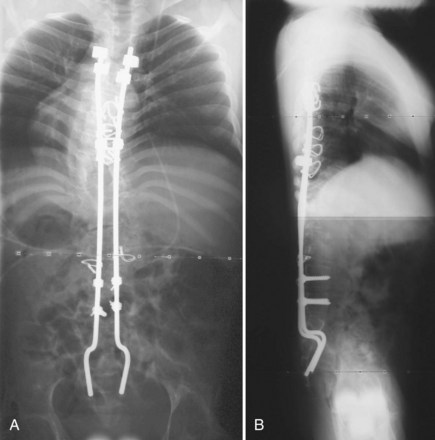
FIGURE 24–11 A and B, Warner-Fackler method of pelvic fixation was used after kyphectomy in this patient with myelodysplasia.
Improvement on the Galveston concept has been the focus of many clinical studies.69,72–74 The use of S1 screws alone was investigated, but bone quality is generally not substantial enough for successful use in patients with neuromuscular scoliosis. Early and colleagues72 compared the biomechanical properties of Galveston sacropelvic fixation versus Colorado II sacropelvic plates using S1 screws, S2 alar screws, and iliac screws and found that both methods provided similar construct stiffness with the Colorado II plate limiting L5-S1 motion in flexion-extension. These authors found that addition of a pair of L1 screws increased the construct stiffness by approximately 50% in both fixation techniques.
The use of iliac screw fixation has become a subject of several more recent articles because of its ease of implantation, avoiding the complex lumbosacral three-dimensional Galveston rod contouring. Clinical and biomechanical studies have shown an improved fusion rate and high pullout strengths after the use of iliac screws for caudad lumbosacral fixation.73,74 In a review of 50 patients treated with one or two bilateral iliac screws, Phillips and colleagues75 concluded that iliac screws provide a safe and effective means to treat neuromuscular scoliosis at 21 months of follow-up. These authors also noted that two screws in each iliac wing provided a more stable fixation with fewer implant-related complications than using a single screw. In a direct comparison of 20 patients with Galveston rod fixation versus 20 patients with iliac screw fixation, Peelle and colleagues76 found that both techniques offer similar pelvic fixation with the iliac screw construct allowing additional screw fixation points to the sacrum and lower lumbar vertebrae. The long-term impact of these screws on the sacroiliac joint was investigated in 67 adult patients by Tsuchiya and colleagues,74 and no evidence of degeneration was observed at 5- to 10-year follow-up.
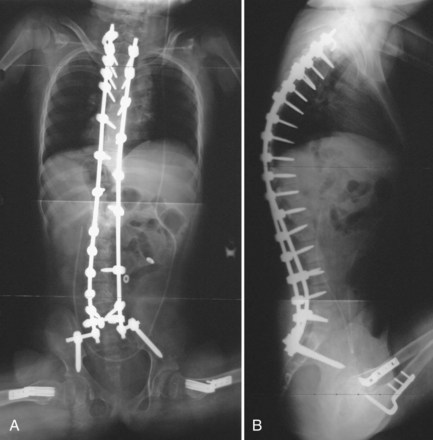
Although iliac screws provide a promising alternative to Galveston fixation, several studies have shown difficulty with implant prominence causing skin irriation.77 Peelle and colleagues76 did not observe this complication in their patient series, however, because they countersunk the screws below the superficial portion of the posterior iliac crest. The patient’s body habitus must be considered when selecting the means of sacropelvic fixation. In very small or thin patients, the authors continue to prefer a Galveston rod construct for pelvic fixation. Screw fixation is used when possible, especially in cases with a kyphotic deformity, where the Galveston rod may not optimally resist pelvic flexion (Fig. 24–12).
When patients with neuromuscular scoliosis are instrumented because of the severe obliquity of the pelvis, intraoperative halo-femoral traction may also be beneficial. Previous studies on this traction technique have been described for patients with idiopathic and congenital scoliosis. In nonambulatory patients with neuromuscular scoliosis, surgeons have relied on rods or screws inserted into the iliac wings by a cantilever method to level the pelvis. This method has the potential to weaken the bone-construct connection in patients with poor bone stock. In a study of 20 nonambulatory patients with neuromuscular scoliosis with halo-femoral traction and 20 matched patients without halo-femoral traction, Takeshita and colleagues78 found that halo-femoral traction provided significantly improved lumbar curve and pelvic obliquity correction at 2-year follow-up. These authors had no associated perioperative complications with this technique and found that unilateral femoral traction with corresponding halo traction was able to level the pelvis to an acceptable position before the surgery was begun. When a significant hip flexion contracture exists, traction results in an increase in lumbar lordosis, however, that may be undesirable.
Some authors have argued that the pelvis can be left unfused in patients with slight pelvic obliquity, mild contractures, and little pelvic deformity in the sagittal plane, whereas others have argued that an ambulatory patient should never be fused to the pelvis.69,79 McCall and colleagues60 advocated that patients with less than 15 degrees of L5 tilt should be considered for a fusion to L5. These authors believed that this fusion allows greater mobility and improves the patients’ ability to carry out activities of daily living. Other studies promote fusion to the pelvis in all patients regardless of ambulatory status. A study by Tsirikos and colleagues58 of ambulatory cerebral palsy patients with severe pelvic obliquity who were treated with fusion to the pelvis by Luque-Galveston instrumentation found that 23 of 24 patients maintained their ambulatory status. Given the progressive nature of this deformity and the fragility of these patients as operative candidates, the authors generally recommend including the pelvis in the fusion mass for most neuromuscular deformities.
Anterior Spinal Release and Fusion
Indications
The addition of an anterior procedure can assist in the correction of neuromuscular spinal deformity and may be justified in several situations (Fig. 24–13). Anterior release and fusion has generally been indicated in patients with rigid scoliosis, patients with rigid kyphosis, immature patients at risk for the development of crankshaft growth, and patients at risk for pseudarthrosis owing to incompetent posterior elements (myelomeningocele or severe osteopenia).80 In assessing the rigidity of the deformity, traction and supine bending films are useful but may underrepresent the available flexibility. An anterior release of a large rigid curve increases the overall spine mobility and makes the posterior correction easier with a relatively high fusion rate. In a study by Newton and colleagues,80 the fusion rate achieved with anterior release combined with posterior corrective instrumentation and fusion was found to be comparable between adolescent patients with neuromuscular scoliosis and idiopathic scoliosis at 3-year follow-up.

Anterior instrumentation and spinal fusion alone and in combination with posterior instrumentation have also been shown to be successful techniques in a subset of patients with neuromuscular scoliosis. The authors’ current algorithm indicates an anterior procedure for “severe” curves (most often thoracolumbar). If a near-complete correction of the major curve can be predicted with anterior instrumentation after an aggressive multilevel discectomy, a single rod anterior system is included. If the curve remains rigid after an anterior release, the anterior instrumentation is skipped, and either an apical vertebrectomy is performed, or the correction is achieved after posterior osteotomies (Fig. 24–14). It is important to avoid “locking in” a poor correction with anterior instrumentation in rigid curves. The goals of achieving a level pelvis and balanced spine must be weighed against the added morbidity of an anterior release or instrumentation procedures or both.

In skeletally immature patients with idiopathic scoliosis, anterior release and fusion reduces anterior overgrowth that results in crankshaft deformity; however, whether this principle can be applied in neuromuscular scoliosis is controversial. In a study of 50 skeletally immature patients with neuromuscular scoliosis treated with posterior instrumentation only, Smucker and Miller81 noted no significant curve progression at an average of 4 years of follow-up. In contrast, Comstock and colleagues,27 after review of 60 skeletally immature patients with cerebral palsy who underwent surgical scoliosis correction, concluded that skeletally immature patients have the best correction and long-term outcomes when treated with anterior and posterior procedures.
Instrumentation
The indications for anterior instrumentation have been a subject of investigation more recently. Several studies have shown that anterior instrumentation alone provides acceptable correction without the need for posterior instrumentation in selected short flexible curves that do not include the pelvis or have less than 15 degrees of pelvic obliquity.82,83 Some studies advocate anterior release followed by posterior instrumentation, whereas others find indications for anterior disc excision and anterior instrumentation before proceeding posteriorly. Anterior instrumentation provides a very powerful means of addressing coronal plane deformities and in many cases simplifies the posterior instrumentation across the levels instrumented anteriorly.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


