reaching a critical mass must be present, and the species and the number of bacteria present must overwhelm host defenses in the particular anatomic site in question. Although random chance may have a role in determining where and when bone and joint infection occurs, specific patterns of infection have been observed that can lead to no other conclusion than that specific factors influence where and in whom musculoskeletal infection occurs.
forming a sequestrum. Because the periosteum retains its blood supply, it remains viable and produces osteoid. The new bone forming around the necrotic sequestrum is known as involucrum. If the metaphysis is intra-articular at the site where infection breaches the metaphyseal cortex, septic arthritis results. Infection generally does not spread down the medullary cavity because the well-developed reticuloendothelial system of the diaphysis is able to prevent its expansion in this direction.
 FIGURE 12-1. A: 12-year-old boy was struck in the distal radius by a hockey puck. Initial radiographs were negative, and the patient’s symptoms completely resolved over 2 weeks. B: Two months later, the patient experienced increasing pain and swelling. Radiographs were repeated and demonstrated a lytic lesion with a sclerotic margin that appeared to cross the physis consistent with osteomyelitis. C: T2-weighted MRI confirms the processes crosses the distal radial physis with cortical breach and adjacent soft-tissue abscess. D: Irrigation and debridement of purulent material was performed, and cultures obtained at surgery confirmed S. aureus osteomyelitis. To reduce risk of persistent infection and to reduce the likelihood of physeal arrest, no bone graft was placed. Two years after surgery, the bone defect has healed, there is no evidence of infection, and the distal radial physis is growing normally. |
cause the treating physician to maintain greater vigilance for subacute osteomyelitis.
concentration of fibrinogen. The ESR result can be affected by the size, shape, and number of erythrocytes present, as well as by other proteins in plasma. Therefore, the ESR is less reliable in the neonate, in the presence of anemia, in patients with sickle cell disease, or when the patient is taking steroids (64, 65).
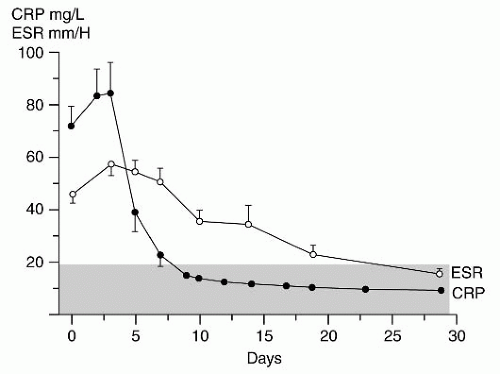 FIGURE 12-2. CRP reaches a peak value more precipitously and has a more rapid return to normal than does the ESR. The stippled area denotes the normal range of values. (Adapted from Unkila-Kallio L, Kallio MJT, Eskola J, et al. Serum C-reactive protein, erythrocyte sedimentation rate, and white blood cell count in acute hematogenous osteomyelitis of children. Pediatrics 1994;93:59-62.) |
promotes binding of a polymerase that replicates the target segment in a series of temperature-dependent cycles. The amplification products are then identified by gel electrophoresis. PCR has produced some promising results in the diagnosis of periprosthetic infections and septic arthritis, but a high falsepositive rate has been reported (75). Recently, success has been reported performing molecular diagnosis of musculoskeletal K. kingae infection by specific, real-time PCR assay (76, 77 and 78). These authors report the K. kingae PCR assays to be reliable and especially helpful in identifying infection caused by this fastidious organism.
temperature, resting pulse rate, ESR, length of hospital stay, and rate of surgical intervention compared to patients with hot scan osteomyelitis.
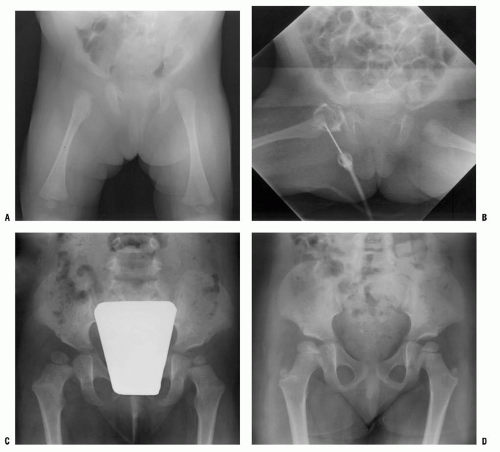 FIGURE 12-3. A: A 2-month-old infant presents following 3 days of increasing irritability, fever, and pseudoparalysis of the right leg. Anteroposterior pelvis radiograph demonstrates widening of the right hip joint space. B: The patient was brought emergently to the operating room, where the right hip was aspirated and an arthrogram was performed to document intraarticular position of the needle. Cell count of the hip joint aspirate was 65,000 per mL; open joint irrigation and debridement of septic arthritis were performed. Cultures later confirm group A Streptococcus infection. C: Two years following open surgical irrigation and drainage, the patient is asymptomatic but A-P pelvis radiograph demonstrates mild hip dysplasia on the right with acetabular index of 25 degrees compared to 22 degrees on the left, 50% femoral head coverage on the right compared to 70% coverage on the left, and widening of the right femoral neck. D: Four years following irrigation and debridement, the right hip dysplasia has improved, with the right acetabular index now measuring 21 degrees and with a femoral head coverage of 70%. Mild coxa magna and femoral neck widening persists. |
or deposition of calcium phosphate. Tumor, trauma, and bone resorption due to disuse may cause increased uptake. The scans may be negative in the first 24 hours of infection before stimulation of bone turnover, and there may be a 4% to 20% false-negative rate with technetium scanning (64). In neonatal infection, the reported sensitivity for technetium scanning has ranged from 30% to 86%, and standard radiography may be more helpful (6, 7, 95). Overall specificity and sensitivity are improved when the scan is interpreted with knowledge of the clinical findings and initial laboratory studies, compared to when the interpretation was a blind reading of the scan (96).
 FIGURE 12-4. A 5-year-old child presents with an increasing limp over 48 hours and with suspected musculoskeletal infection. History and physical examination do not localize the process. ESR and CRP are elevated. A: The lateral (as well as the anteroposterior) radiograph of the spine is normal. B: Technetium bone scan shows increased isotope uptake in the L4 and L5 vertebral bodies suggestive of discitis, but neoplasm cannot be excluded. C: T2-weighted MRI helps confirm the diagnosis of discitis, demonstrating that the process is centered in the L4-L5 disc with no evidence of neoplasm, bone, soft tissue, or epidural abscess. Intravenous followed by oral antibiotic treatment was initiated, with complete resolution of symptoms after antibiotic therapy duration of 3 weeks. D: Final follow-up 3 years later demonstrates a normal lumbar spine radiograph in the asymptomatic patient. |
with suspected osteomyelitis or septic arthritis and found that iatrogenic soft tissue and bone edema related to recent surgery in children with suspected osteomyelitis or septic arthritis has minimal effect on diagnostic accuracy of MRI (108). Spiegel et al. (109) at Children’s Hospital of Philadelphia evaluated the usefulness of MRI as a routine follow-up test used to assess surgical treatment of musculoskeletal infection and noted that if patients’ clinical course was unremarkable, MRI did not add clinically significant additional information. From these two studies, we can conclude that if patients demonstrate clinical improvement with treatment, then routine follow-up MRI is not necessary, but if the treatment course is complicated by clinical evidence of persistent or recurrent infection, then MRI can provide helpful, reliable information that is not degraded by previous surgery.
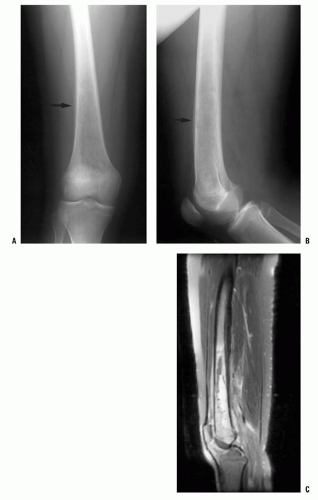 FIGURE 12-5. MRI may be very helpful when differentiating between osteomyelitis and primary bone malignancy. A,B: This 12-year-old female patient was referred for evaluation of femoral osteosarcoma. The standard anteroposterior and lateral radiograph shows periosteal reaction along the distal one-third of the femur, consistent with primary bone sarcoma or osteomyelitis (arrows). C: T2-weighted MRI without contrast demonstrates preservation of some normal marrow fat within the intramedullary canal and a fluid-filled abscess cavity diagnostic of osteomyelitis. Diffuse inflammation is present in adjacent soft tissues without a discrete soft-tissue mass. Osteomyelitis was confirmed at surgery. |
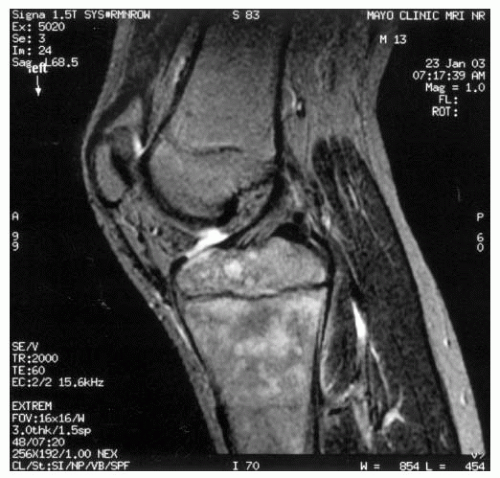 FIGURE 12-6. This 13-year-old male presents with a 4-month history of proximal tibial pain and normal plain film radiographs. Lateral T2 MRI without contrast lacks the high signal intensity associated with marrow edema caused by osteomyelitis and suggests a more indolent cause. MRI is the only imaging modality that can provide such detailed information. Biopsy established the diagnosis of a diffuse, large B-cell lymphoma. |
of the process, then technetium bone scintigraphy is an appropriate next imaging study (Fig. 12-4). If additional imaging is needed to establish a diagnosis or characterize a pathologic process once the process has been localized, then MRI is the imaging study of choice to provide maximal information about the bone and soft-tissue pathology. For straightforward musculoskeletal infection in the appendicular skeleton, MRI is often not necessary; but for patients whose history, examination, laboratory evaluation, and plain film radiographs are not concordant, or for patients with suspected infection of the pelvis or axial skeleton, MRI is a very helpful imaging study.
TABLE 12-1 Synovial Fluid Analysis | |||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||
had a cell count of >50,000 per mL. Brucella melitensis was recovered from the synovial fluid culture in all patients (119).
thought to be a postinfectious arthritis. Both may present with a history of a few to several days of hip pain and with limp progressing to the inability to walk. The physical signs are similar in both, with limited and painful internal rotation, abduction, and extension. A longer history of symptoms, with cyclic improvement and worsening, suggests toxic synovitis. The pain is usually worse and the motion more restricted in septic arthritis.
TABLE 12-2 Empiric Antibiotic Treatment Recommendations for Musculoskeletal Infection | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
appropriate intravenous antibiotic. Similar to the antibiotic treatment of septic arthritis, the administration route and the duration of treatment of AHO are controversial and depend upon the clinical situation of each patient. At one time, nearly all children with AHO were routinely treated with 6 weeks of intravenous antibiotics as a hospital inpatient. Over the last two decades, several trends have developed: (a) treatment has moved from inpatient to an outpatient setting and (b) treatment has shifted from entirely parenteral to a parenteral then oral antibiotic regimen. Intravenous therapy is initiated in the hospital setting, but once therapeutic response to treatment is confirmed, conversion to oral antibiotic treatment is made and continued on an outpatient basis.
TABLE 12-3 Antibiotics Commonly Used in the Treatment of Bone and Joint Sepsis | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
necrotic sequestrum. A valuable general treatment principle is to aggressively debride the necrotic sequestrum but to leave in place the viable involucrum.
1. Recurrent/persistent infection despite a course of reasonable and appropriate treatment
2. Extensive chronic infection that cannot be completely débrided surgically
3. Extensive osseous defects and dead space to be treated by delayed bone grafting (Fig. 12-7)
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


