Chapter 96 Glycyrrhiza glabra (Licorice)
Glycyrrhiza glabra (family: Leguminosae)
Common names: licorice, glycyrrhiza
 General Description
General Description Chemical Composition
Chemical Composition
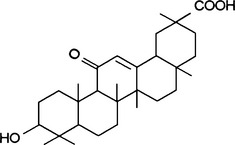
The major active component of licorice root is the triterpenoid saponin glycyrrhizin (also known as glycyrrhizic acid or glycyrrhizinic acid; Figure 96-1), which is usually found in concentrations ranging from 6% to 10%. The intestinal flora is believed to hydrolyze glycyrrhizin, yielding the aglycone molecule (glycyrrhetinic acid) and a sugar moiety, resulting in absorption of both.1
A processed licorice extract, deglycyrrhizinated licorice (DGL), which is used in the treatment of peptic and aphthous ulcers, is made by removing the glycyrrhizin molecule. The active components of DGL are flavonoids. These compounds demonstrated impressive protection against chemically-induced ulcer formation in animal studies.2
Other active constituents of licorice include isoflavonoids (e.g., isoflavonol, kumatakenin, licoricone, glabrol); chalcones; coumarins (e.g., umbelliferone, herniarin); triterpenoids; and sterols, lignins, amino acids, amines, gums, and volatile oils.3
 History and Folk Use
History and Folk Use
The medicinal use of licorice in both Western and Eastern cultures dates back several thousand years. It was used primarily as a demulcent, expectorant, antitussive, and mild laxative. Licorice is one of the most popular components of Chinese medicines. Its traditional uses include treating peptic ulcers, asthma, pharyngitis, malaria, abdominal pain, insomnia, and infections.3
 Pharmacology
Pharmacology
Licorice is known to exhibit many pharmacologic actions, including the following3:
The majority of these actions are discussed individually later. Although much of the pharmacology focuses on glycyrrhizin and glycyrrhetinic acid, it is worth remembering that licorice has many other components, such as flavonoids, which may have significant pharmacologic effects.
Estrogenic Activity
Most herbalists generally believe that glycyrrhiza exhibits alterative action on estrogen metabolism (i.e., when estrogen levels are too high, it inhibits estrogen action, and when estrogens are too low, it potentiates estrogen action when used in greater amounts).4 Glycyrrhetinic acid has been shown to antagonize many of the effects of estrogens, particularly exogenous estrogens.5 The estrogenic action of glycyrrhiza is due to its isoflavone content, as many isoflavone structures (e.g., daidzein and genistein from soy) are known to possess estrogenic effect. The estrogenic activity of the isoflavones appears to be more significant than the estrogen antagonism of glycyrrhetinic acid.6 Interestingly, these same components inhibit breast cancer cell growth.7
Pseudoaldosterone Activity
Long-term ingestion of glycyrrhiza in large doses leads to a well-documented pseudoaldosteronism syndrome (i.e., hypertension, hypokalemia, sodium and water retention, low plasma renin activity, and suppressed urine and serum aldosterone levels).8–13 In normal subjects, the amount of glycyrrhizin needed to produce these side effects is between 0.7 and 1.4 g, which corresponds to approximately 10 to 14 g of the crude herb.9 Although glycyrrhiza possesses mineralocorticoid activity (about four orders of magnitude lower than aldosterone) and binds to aldosterone receptors, it is largely without effect in adrenalectomized animals or in patients with severe adrenocorticoid insufficiency. Therefore, it can be concluded that its primary effects are largely as a result of glycyrrhetinic acid inhibiting the breakdown of aldosterone in the liver.14 Glycyrrhizin and glycyrrhetinic acid were shown to suppress 5-β-reductase, the main enzyme in humans responsible for inactivating cortisol, aldosterone, and progesterone. These effects can be put to good use in the treatment of Addison’s disease, a severe disease of adrenal insufficiency.13
Antiinflammatory and Antiallergic Activity
Glycyrrhiza has significant antiinflammatory and antiallergic activity.15,16 Although both glycyrrhizin and glycyrrhetinic acid bind to glucocorticoid receptors, and much of glycyrrhiza’s anti-inflammatory activity has been explained by its “cortisol-like effects,” many of the effects of glycyrrhiza actually antagonize or counteract cortisol.17 Antagonism to such actions of cortisol include activation of tryptophan oxygenase, accumulation of hepatic glycogen, stimulation of hepatic cholesterol synthesis, inhibition of thymus atrophy, and inhibition of adrenocorticotropic hormone synthesis and secretion. Glycyrrhizin does, however, reinforce cortisol’s inhibition of antibody formation, stress reaction, and inflammation. Like its mineralocorticoid effect, glycyrrhiza’s major influence on glucocorticoid metabolism is probably related to its suppression of 5-β-reductase activity, thus increasing the half-life of cortisol. Glycyrrhetinic acid can also increase the conversion of cortisol to the more powerful cortisone.18
Glycyrrhiza’s major cortisol-like effect relates to its ability to inhibit phospholipase A2.19 This enzyme is responsible for cleaving lipids from biomembranes for eicosanoid metabolism. In addition to this effect, glycyrrhizin was also shown to inhibit cyclic adenosine monophosphate phosphodiesterase, thereby raising cyclic adenosine monophosphate levels and prostaglandin formation by activated peritoneal macrophages from rats.20,21 Glycyrrhizin was shown to inhibit experimentally induced allergenic reactions, such as the Arthus phenomenon, the Shwartzman phenomenon, and Forssman anaphylaxis, and to be an antidote against many toxins, including diphtheria, tetanus, and tetrodotoxin.21,22
Glycyrrhizin exerts antithrombotic effects but does not potentiate the inhibitory activity of antithrombin III or heparin cofactor II toward thrombin.23
Immunostimulatory and Antiviral Effects
Glycyrrhizin and glycyrrhetinic acid were shown to induce interferon.24 The induction of interferon leads to significant antiviral activity, because interferons bind to cell surfaces, where they stimulate synthesis of intracellular proteins that block the transcription of viral DNA. The induction of interferon is also followed by activation of macrophages and augmentation of natural killer cell activity.
Glycyrrhizin was shown to directly inhibit the growth of several DNA and RNA viruses in cell cultures (vaccinia, Epstein-Barr, Herpes simplex, Newcastle disease, vesicular stomatitis viruses, severe acute respiratory syndrome [SARS]-associated coronavirus, and HIV) and to inactivate herpes simplex virus 1 (HSV-1) irreversibly.25–28 Administration of glycyrrhizin to mice with herpetic encephalitis increased their survival rate on average about 2.5 times, whereas it reduced HSV-1 replication in the brain to 45.6% of the controls.29 Glycyrrhizin, as stated earlier, also inhibited the thymolytic and immunosuppressive action of cortisone. Other licorice components exerted immunomodulatory effects as well.30
Anticancer Effects
Licorice components exert a wide range of anticancer effects.31 The most active appear to be the flavonoids and coumarins. For example, isoliquiritigenin was shown to suppress colon cancer in mice via markedly decreasing both prostaglandin E2 and nitric oxide production in mouse macrophage cells.32 Isoliquiritigenin was also shown to significantly inhibit the proliferation of prostate and breast cancer cell lines in dose- and time-dependent manners.7,33 Isoliquiritigenin also significantly reduced pulmonary metastasis in mouse renal cell carcinoma and prevented the leukocytopenia caused by administration of 5-fluorouracil.34 A coumarin compound, identified as licocoumarone, was shown to be the factor in licorice that induces apoptosis.35
Antibacterial Activity
Alcohol extracts of glycyrrhiza displayed antimicrobial activity in vitro against Helicobacter pylori, Staphylococcus aureus (including antibiotic resistant strains), Streptococcus mutans, Mycobacterium smegmatis, Bacillus subtilis, S. pyogenes, Haemophilus influenzae, Moraxella catarrhalis, and Candida albicans.36–39 The majority of the antimicrobial effects are due to isoflavonoid components, with the saponins having a lesser antibacterial effect.
Antihepatotoxic Activity
Glycyrrhetinic acid inhibits carbon tetrachloride and galactosamine-induced liver damage. The mechanism of action is prevention of nonenzymatic lipid peroxidation and inhibition of the production of free radicals by the enzymatic action of nicotine adenine disphosphonucleotide, reduced–cytochrome P450 reductase on CCl4.40
Memory-Enhancing Effect
Licorice may exert some memory-enhancing effects. In a study in mice, licorice was shown to enhance learning and memory in mice as determined by the elevated plus-maze and passive avoidance paradigm. Furthermore, licorice significantly reversed the amnesia induced by diazepam and scopolamine. Although anti-inflammatory and antioxidant properties may contribute favorably to the memory-enhancement effect, because scopolamine-induced amnesia was reversed as well, it is possible that the beneficial effect on learning and memory was due to facilitation of cholinergic transmission.41
 Clinical Applications
Clinical Applications
• Use of oral licorice preparations containing glycyrrhizin
• Use of licorice flavonoid oil (LFO)
• Use of topical preparations containing glycyrrhetinic acid
 Deglycyrrhizinated Licorice
Deglycyrrhizinated Licorice
Although glycyrrhetinic acid was the first drug proven to promote healing of gastric and duodenal ulcers,43 most physicians using licorice in the treatment of peptic ulcers now use DGL. DGL was actually shown to be more effective than glycyrrhetinic acid, without side effects.44
Rather than inhibit the release of acid, DGL stimulates the normal defense mechanisms that prevent ulcer formation and stimulate healing of the damaged mucous membranes. Specifically, DGL increases the following45,46:
• The blood supply to the damaged mucosa
• The number of cells producing the mucus that protects the mucous membranes
• The amount of mucus the cells produce
In addition, several flavonoid components of G. glabra have shown significant activity against H. pylori, including antibiotic-resistant strains.38
Gastric Ulcers
Numerous clinical studies over the years found DGL to be an effective antiulcer compound. DGL was shown to be extremely effective in the treatment of gastric ulcers.47–51 In one study, 33 gastric ulcer patients were treated with either DGL (760 mg, three times a day) or a placebo for 1 month.50 There was a significantly greater reduction in ulcer size in the DGL group (78%) than in the placebo group (34%). Complete healing occurred in 44% of those receiving DGL, but only in 6% of the placebo group.
In several head-to-head comparison studies, DGL was shown to be more effective than cimetidine (Tagamet), ranitidine (Zantac), or antacids in both short-term treatment and maintenance therapy of peptic ulcers.47,48,52 However, although these drugs are associated with significant side effects (see preceding section), DGL is extremely safe and is only a fraction of the cost.
Subsequent studies showed DGL to be as effective as Tagamet and Zantac for both short-term treatment and maintenance therapy of gastric ulcer.47–49 For example, in a head-to-head comparison with Tagamet, 100 patients received either DGL (760 mg, three times a day between meals) or Tagamet (200 mg, three times a day, and 400 mg at bedtime).48 The percentage of ulcers healed after 6 and 12 weeks were similar in both groups. Although Tagamet is associated with some toxicity, DGL is extremely safe to use.
Gastric ulcers are often a result of using alcohol, aspirin, or other nonsteroidal anti-inflammatory drugs, caffeine, and other factors that decrease the integrity of the gastric lining. Because DGL was shown in human studies to reduce the gastric bleeding caused by aspirin, DGL is strongly indicated for the prevention of gastric ulcers in patients requiring long-term treatment with ulcerogenic drugs such as aspirin, nonsteroidal anti-inflammatory agents, and corticosteroids.51
Duodenal Ulcers
DGL is also effective in duodenal ulcers. This is perhaps best illustrated by one study in patients with severe duodenal ulcers: 40 patients with chronic duodenal ulcers of 4 to 12 years’ duration and more than six relapses during the previous year were treated with DGL.53 All of the patients were referred for surgery because of relentless pain, sometimes with frequent vomiting, despite treatment with bed rest, antacids, and anticholinergic drugs. Half of the patients received 3 g/day of DGL for 8 weeks; the other half received 4.5 g/day for 16 weeks. All 40 patients showed substantial improvement, usually within 5 to 7 days, and none required surgery during the 1-year follow-up. Although both dosages were effective, the higher dosage was significantly more effective than the lower dosage.
In another more recent study, the therapeutic effect of DGL was compared with that of antacids or cimetidine in 874 patients with confirmed chronic duodenal ulcers.52 Ninety-one percent of all ulcers healed within 12 weeks; there was no significant difference in healing rate in the groups. However, there were fewer relapses in the DGL group (8.2%) than in those receiving cimetidine (12.9%) or antacids (16.4%). These results, coupled with DGL’s protective effects, suggest that DGL is a superior treatment of duodenal ulcers.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


