CHAPTER 31 Complications of Shoulder Arthroscopy
The first large-scale report of complication rates was by Small1 in 1986, which included 14,329 shoulder arthroscopic procedures. He noted an overall complication rate of 5.3% with staple capsulorrhaphy but only 0.76% with subacromial surgery. This early study demonstrated the relative safety of shoulder arthroscopy but was limited to relatively simple procedures. Multiple other reviews have been reported since then, but the numbers are difficult to compare for a number of reasons, including differing definitions of what actually constitutes a complication. Berjano and colleagues2 reported on 179 shoulder arthroscopic procedures, noting an overall complication rate of 9.49%. They stated that in procedures that combined arthroscopy with an open procedure, the complication rate was 5.26% versus 10.63% in arthroscopic procedures alone. Interestingly, they did not define shoulder stiffness as a postoperative complication and also noted that few of the complications were serious. Muller and associates3 reported on 846 shoulder arthroscopic procedures, with an overall complication rate of 5.8%. Of the complications in this series, 43% were caused by infections.
What does appear to be consistent across the literature is that the overall complication rate has remained stable, even in the face of the ever-increasing complexity of arthroscopic procedures. Most reviews place this number between 5.8% and 9.5%.1–5 This may be to the result of improvements in arthroscopic instrumentation, techniques, and implants, as well as a better understanding of shoulder pathology and function. These advancements may help offset the potential for increased complication rates associated with more complex procedures. Standardized postoperative rehabilitation programs also have likely decreased some of the complications seen in shoulder arthroscopy.
GENERAL COMPLICATIONS
The incidence of infection after shoulder arthroscopy is low. This may be due to the result of the copious amount of irrigation that is constantly run through the shoulder during the procedure, as well as the minimal exposure of deep tissues to the environment. D’Angelo and Ogilvie-Harris6 reported on 9 cases of septic arthritis after arthroscopy, with an incidence of 0.23%. Based on their studies, they recommended routine antibiotic prophylaxis to prevent these potentially serious complications. Bigliani and coworkers7 reviewed the literature in 1991 and noted infection rates from 0.04% to 3.4%. Other reviews have noted similar infectious rates.2,4 Brislin and colleagues8 published a recent study on 263 patients who had undergone arthroscopic rotator cuff repair; they noted only a single infection in this group, with an incidence of 0.38%. Athwal and associates,9 in 2007, reported on 39 cases of deep infection after rotator cuff repair. They noted that long-term functional limitations in these patients are not uncommon. They emphasized recognizing Propionibacterium acnes as the most likely causative organism and the need for at least 7 days of culture to identify this organism. P. acnes has also been implicated as a potential causative factor for the onset of chondrolysis after shoulder arthroscopy and therefore should be treated aggressively. Regardless of the true incidence, infection after shoulder arthroscopy requires a high index of suspicion with prompt management once deep infection is recognized.
General anesthetic complications germane to any surgical procedure also apply to shoulder arthroscopy. In addition, fatal air embolism10 and pneumothorax,11 possibly related to the use of CO2, pulmonary edema,12 and pneumomediastinum13 have all been reported during shoulder arthroscopic procedures. It is important to educate patients about these risks for them to understand that minimally invasive procedures can still be associated with significant complications.
Of special relevance to shoulder arthroscopy is the increasing use of interscalene anesthesia for intraoperative pain management and postoperative pain control (Fig. 31-1). Although purported to be a safe and effective means for pain control, reports of seizures, cardiovascular collapse, and severe respiratory distress have been noted. Additionally, neurologic complications in the form of transient and even permanent brachioplexopathies are a known risk of regional brachial plexus blockade.14,15 Lenters and coworkers16 have reviewed the experience of a single medical center over a 15-year period and supplemented this data with records from the national American Society of Anesthesiology Closed Claims Database. From the hospital experience, they reported a total of 41 major complications following interscalene block, with 14 of them still present, affecting comfort and function at the most recent follow-up. From the database, they noted 19 permanent complications and 4 deaths attributable to interscalene brachial plexus block. It appears that fewer complications arise as anesthesiologists become more experienced with the techniques and with the use of newer technologies, including ultrasound-guided blocks. However, complications can and do still occur. It is important that the anesthesiologists performing these procedures have significant experience and understand the risks, and that they communicate these to the patients. These procedures must be performed with the patient awake. Ultrasound guidance to direct needle placement is expected to decrease the risk of interscalene blocks.

Deep venous thrombosis (DVT) of the lower extremity after shoulder arthroscopy has rarely been noted in the literature.17,18 Although there have only been a few reported cases of life-threatening pulmonary embolism (PE), the prevalence of these complications are likely much more common than once thought. Standard precautions, such as using mechanical compression devices on the lower extremities during the procedure and early mobilization, may minimize the risk. Currently, there are no guidelines in place suggesting that the use of routine chemoprophylaxis is indicated after shoulder arthroscopy.
COMPLICATIONS SPECIFIC TO SHOULDER ARTHROSCOPY
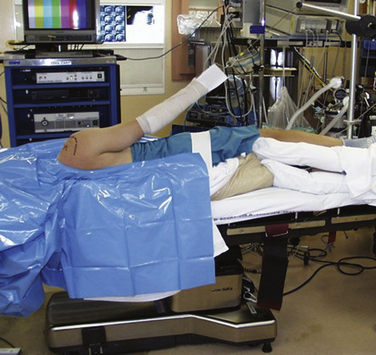
Complications resulting from the two prevalent patient positions used during arthroscopy do occur. In the lateral decubitus position (Fig. 31-2), traction neuropraxia has been reported to occur up to 10% of the time.19 In 1987, Klein and colleagues20 placed strain gauges on the brachial plexus of cadavers and measured the strain on the plexus in the lateral decubitus position with varying amounts of flexion and abduction. They found that increasing flexion and abduction decreased strain on the brachial plexus. Stanish and Peterson21 have reviewed the literature on neurologic injuries after shoulder arthroscopy and suggested that careful patient positioning, minimal traction to distract the joint (no more than 7 kg), limiting the length of the procedure, and accurate portal positioning could minimize neurovascular complications.
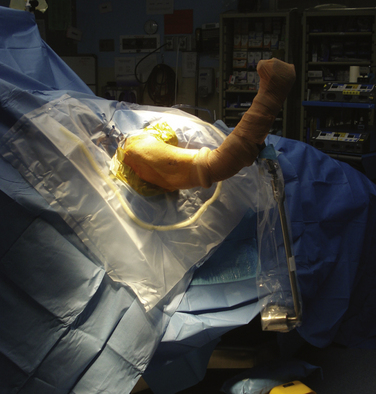
The beach chair position (Fig. 31-3) was described in 1988 by Skyhar and associates.22 Its advantages include easier airway access, placing the anatomy in the standard upright position, the ability to move the arm into different positions intraoperatively and decreased risk of traction-related neuropraxia. Several reports of catastrophic complications have been reported recently with the use of the beach chair position. Pohl and Cullen23 reported on four cases of shoulder surgery in the beach chair position that resulted in death in one patient and severe brain damage in three others. Stroke, brain death, loss of vision, and ophthalmoplegia have also been described.24,25 These complications are thought to be attributable to errors in blood pressure reference points leading to decreased cerebral perfusion. In 2008, Papadonikolakis and coworkers26 reviewed the literature and suggested using invasive blood pressure monitoring or placing a blood pressure cuff around the contra lateral brachium (at the level of the heart) to avoid erroneous pressure numbers. Currently, it appears that the choice of position should be left up to the surgeon. Recognition of the potential complications of the preferred position and taking preventative measures can minimize the occurrence of a significant untoward event.
With the increasing complexity of arthroscopic procedures about the shoulder, the need to establish portals that allow for optimal access and precision placement of implants has also increased. Although vascular complications associated with portal placement remain rare,4,27 direct neurologic injury remains a concern. Segmuller and colleagues28 noted direct cutaneous nerve injury in 7% of their 304 patients undergoing shoulder arthroscopy. Most of these injuries involved a cutaneous branch of the axillary nerve at the site of the established lateral portal. This concern over direct nerve injury underscores the importance of accurate portal placement. In 2004, Lo and associates29 studied the neurovascular anatomy in proximity to the most commonly used arthroscopic portals established via an outside-in approach. They noted that with the exception of the cephalic vein, all the neurovascular structures were more than 20 mm away from all the portals evaluated; it was concluded that the standard and accessory arthroscopic portals are safe when established in an outside-in fashion. Other considerations such as careful palpation of bony landmarks, accurate knowledge of shoulder anatomy, accounting for fluid extravasation, and the use of cannulas during portal placement may enhance safety during shoulder arthroscopy.
Iatrogenic tendon injury has been described in the literature. Norwood and Fowler30 described this complication in 1989. The port of Wilmington portal is an accessory portal used primarily for repair of posterior and posterior-superior labral tears. Proper placement of the portal leads to penetration of the muscular portion of the supraspinatus. However, if improperly placed, injury to the tendinous portion of the supraspinatus can occur. It appears that accurate portal placement and a thorough understanding of shoulder anatomy can minimize this complication.
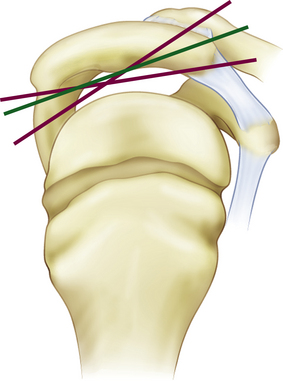
Fractures of the acromion, clavicle, and humerus can occur during shoulder arthroscopy. Fracture of the acromion has been extensively described in the literature.4,5,31 This is usually a result of overzealous and inaccurate resection of the acromial spur, often in the setting of a patient with a thin acromion preoperatively (Fig. 31-4). Simple precautions can be taken to prevent this complication. Measurement of the thickness of the acromion on preoperative radiographs and attention to the depth of resection using the known diameters of the arthroscopic tools as a reference are helpful (Fig. 31-5). Additionally, adequate visualization and exposure of the anterior acromion to prevent beginning the resection too far posteriorly, as well as working from anterior-inferior to superior, will further minimize the chance of excessive resection. Fractures can be treated with screw fixation, tension band fixation, or excision of the remaining bone and repair of the deltoid attachment. Clavicle fractures can occur as a result of the surgeon becoming disoriented during subacromial surgery. At this point, the surgeon may mistakenly resect through the shaft of the clavicle instead of the acromioclavicular (AC) joint because of straying too medially during the procedure. Humeral fractures are also a concern during shoulder arthroscopy. Humeral neck or shaft fractures can occur as a result of excessive manipulation of a stiff shoulder (Fig. 31-6). Greater tuberosity fractures may follow improper instrument penetration (Fig. 31-7) or implant placement. Paying attention to the amount of force imparted during manipulation and careful attention to instrument placement and topography of the tuberosity can minimize the risk of these complications. When such a fracture occurs, it can be treated conservatively or by reduction and internal fixation, depending on the stability of the fracture.