Most cases of CMF occur in the metaphysis of tubular bones of the lower extremity.
Approximately one-third of the cases are diagnosed around the knee joint, especially the proximal tibial metaphysis which is the most common site of involvement and followed by the distal femoral metaphysis.
Rarely there are reports of cases that involve cortical bones.
Small bones of the feet are among the frequently involved site.
Upper extremity involvement is rare.
In the pelvis, the ilium is the most frequent site of involvement.
Other than that, there were reports to occur in the craniofacial bones, ribs, spine, clavicle, calcaneus, and sternum.
Clinical Symptoms and Signs
Clinically, patients present with pain that can persist for several months to several years or local swelling.
On very rare occasions, they suffer from rickets which is reported as an oncogenic osteomalacia.
Image Diagnosis
Radiographic Features
Mainly located in the metaphysis of long tubular bones and appears as a sharply circumscribed radiolucent lesion with an elongated shape of varying size of about 2–10 cm in largest diameter. Cortical expansion, exuberant endosteal sclerosis, and coarse trabeculation can be seen (Figs. 22.1 and 22.2).
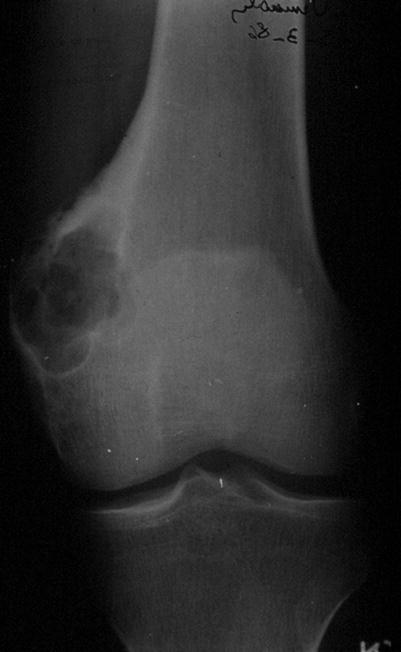
Fig. 22.1
The radiograph of the distal femur shows an expansile osteolytic metaphyseal lytic lesion
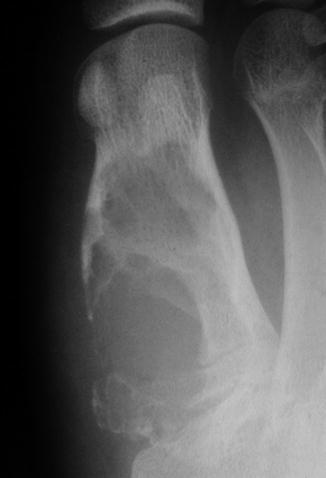
Fig. 22.2
The radiograph shows a well-defined osteolytic bone lesion at the first metatarsal bone. The cortical margin is partially disrupted at the medial margin
Extensive periostitis and pathological fracture are rare, and calcification is infrequent.
The lesion is sharply defined and eccentrically located. Large lesions can be seen as hemispheric osseous defects with destruction of cortex.
Chondromyxoid fibroma arising in a flat bone may show irregular contours with osteolysis and bone expansion (Fig. 22.3).
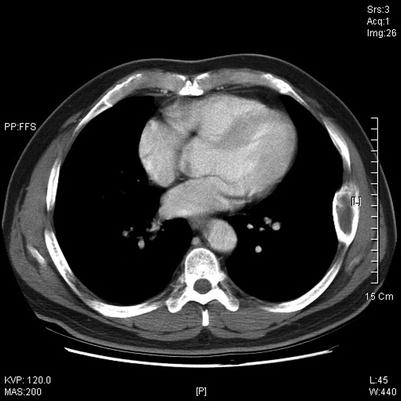
Fig. 22.3
CT scan shows large irregular osteolytic and expansile lesion in a rib
CT Features
At CT, the extent of bone involvement can be better evaluated.
MRI Features
On MRI, chondromyxoid fibroma shows a multilobulated pattern, with low signal intensity on T1-weighted images and high signal intensity on T2-weighted images. With contrast injection, the central portion of the lesion may show no enhancement due to the myxoid component.
Image Differential Diagnosis
Chondrosarcoma
Chondrosarcoma may be mistaken for chondromyxoid fibroma and vice versa, especially if the lesion involves the pelvic bones. Chondrosarcoma usually has a more aggressive picture, is poorly circumscribed, and contains calcification.
Fibrous Dysplasia
FD shares, in numerous cases, the peripheral sclerosis seen in CMF, but the lesion is denser, with the so-called ground glass appearance in the center.
Pathology
Gross Features
Most often, CMF has been treated by curettage, so it is not usual to observe an intact gross specimen.
Curettage specimens are composed of a blue-gray or white tissue that rarely shows necrosis, cystic change, or liquefaction (Fig. 22.4).

Fig. 22.4
Gross features of chondromyxoid fibroma show yellow-white lobulated appearance
Typical hyaline cartilage is not present.

Histological Features
CMF has distinct microscopic features characterized by variably sized sharply demarcated lobules. These lobules vary in size, ranging from easily visible under low-power view to smaller ones (Fig. 22.6). The lobules tend to be hypocellular centrally with greater cellularity at the periphery (Fig. 22.7).
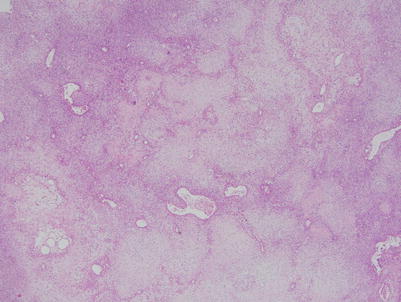
Fig. 22.6
Low power of chondromyxoid fibroma shows characteristic lobular configuration, relatively hypocellular and peripheral hypercellular areas
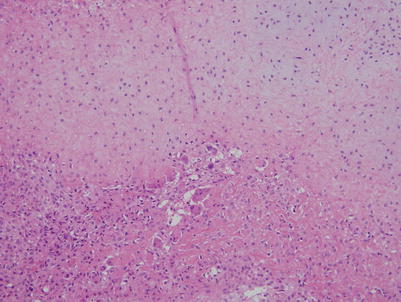
Fig. 22.7
At the periphery of the lobule, there are giant cells and mononuclear cells showing oval to spindle nuclei and pink cytoplasm
The lesional cells are spindled to stellate and are distributed in an abundant extracellular chondroid matrix (Fig. 22.8). Frequently, there is abundant pink cytoplasm, producing an epithelioid appearance (Fig. 22.9).
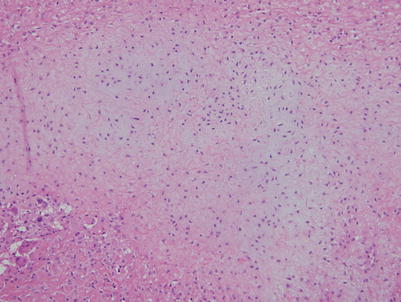
Fig. 22.8
In the lobule, elongated or stellate cells present in an abundant extracellular chondroid matrix
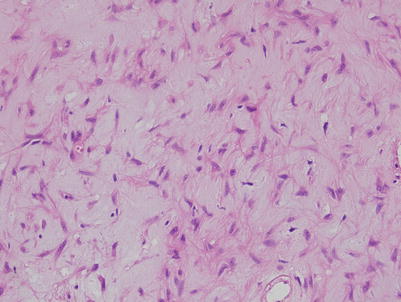
Fig. 22.9
At higher magnification, the central portion of tumor shows elongated to spindle, stellate cells admixed with myxoid stroma
The lobules are separated by fibrous bands (Fig. 22.10). The fibrous bands contain blood vessels and giant cells.
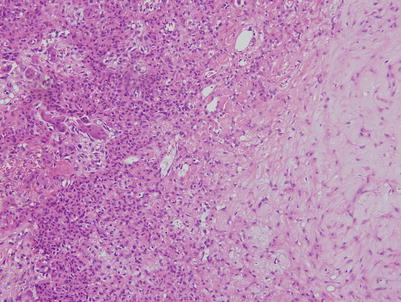
Fig. 22.10
The peripheral cells are more spindled to polyhedral shaped, simulating chondroblastoma, and appear to separate the lobules by fibrous bands
Approximately 50 % of CMF cases have scattered benign giant cells. Large bizarre hyperchromatic nuclei can be seen in 20–30 % of cases; however, they are usually focal and associated with large amounts of cytoplasm, sometimes with smudgy or degenerative features.
Mitoses are extremely rare in CMF, and atypical mitoses have not been noted.
Microscopic cystic or liquefactive change is uncommon and is usually focal, when present. Well-formed hyaline cartilage is present in less than 20 % of cases.
Calcification is present in about one third of cases, as either fine granules or denser and plaques (Fig. 22.11). Hemosiderin deposition is present at the lobular periphery associated with inflammatory cells and lymphocytes.
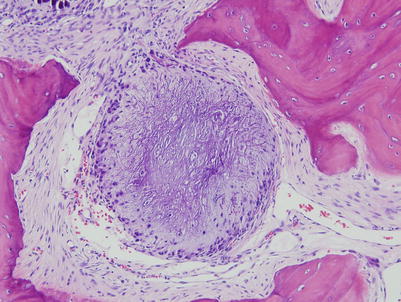
Fig. 22.11
Occasionally, this type of coarse calcification in the lobule is presentRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








