CHAPTER 18 Arthroscopic Fusion for Degenerative Arthritis of the Subtalar Joint
Arthrodesis of the subtalar joint is an accepted treatment option for many problems of the hindfoot, such as post-traumatic and primary arthritis, posterior tibial tendon dysfunction, symptomatic congenital deformities, and inflammatory arthritis.1–3 Although sometimes viewed as a salvage procedure, results from subtalar fusions have been reported to be good or excellent in many patients.4–6
The many advantages of isolated subtalar arthrodesis compared with triple arthrodesis and other salvage procedures have been recognized. The major advantage of isolated fusion compared with triple arthrodesis or pantalar arthrodesis is that isolated subtalar fusion preserves motion in adjacent joints.7 In a study of 48 isolated subtalar arthrodeses, Mann found that preserving motion of the transverse tarsal joints decreased the incidence of clinically significant symptoms of arthritis.6
ANATOMY
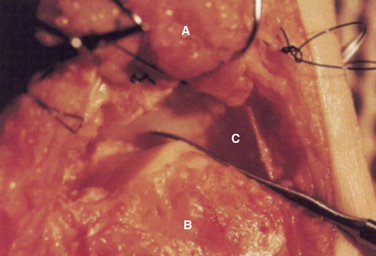
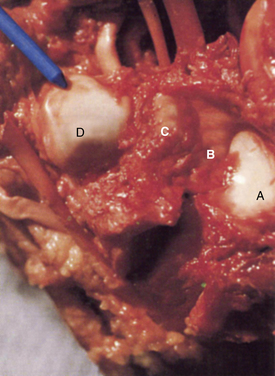
The subtalar joint is composed of three articulations: the posterior, middle, and anterior joints or facets (Figs. 18-1 and 18-2). Several extra-articular ligaments stabilize the subtalar joint. The major ligaments encountered during subtalar arthroscopy are the intra-articular components, which consist of the interosseous, lateral, and anterior talocalcaneal ligaments. These components coalesce to form the division between the posterior and the middle facets of the subtalar joint. The interosseous ligament is a broad, stout structure that is approximately 2.5 cm wide from its medial to lateral side. It marks the arthroscopic boundary for posterior subtalar arthroscopy.
Open subtalar arthrodesis has historically been the fusion method of choice, and results have generally been favorable. Studies reporting the results of open fusion techniques have all described similar results for fusion rate, time to union, and complications, such as nonunion or malunion, infection, and symptomatic hardware problems.8–12 Open procedures entail removal of the interosseous ligaments and their vasculature and a lateral incision that can result in nerve dysfunction. Nonunion rates of 5% to 16% have been reported.4,6 The successful results of arthroscopic ankle fusion have stimulated the development of an arthroscopic approach for subtalar joint arthrodesis, which has the advantages of reduced perioperative morbidity and preservation of the blood supply.13–15
Arthroscopic subtalar arthrodesis was designed to improve traditional methods by using a minimally invasive technique. Subtalar arthroscopy has been described by several investigators, but few reports of arthroscopic subtalar fusion have been published.16 The development of an arthroscopic technique for subtalar arthrodesis was intended to lower morbidity using techniques and principles similar to those used for arthroscopic ankle fusion. It was hypothesized that perioperative morbidity could be reduced, blood supply preserved, and proprioceptive and neurosensory input enhanced. These theoretical advantages prompted us to initiate a prospective study to document the effectiveness of the procedure and to determine the time until complete fusion, the incidence of delayed unions and nonunions, and the incidence of complications.
PATIENT EVALUATION
Diagnostic Imaging
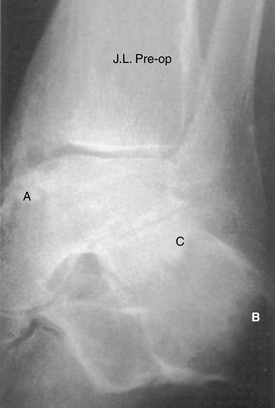
Evaluation for subtalar pathology should include plain radiographs of the ankle and subtalar joints. The Broden view provides the best visualization of the posterior subtalar joint and may be sufficient to confirm the diagnosis of subtalar pathology (Fig.18-3). Profound degenerative radiographic changes in the joint are not needed to confirm a diagnosis, because only small alterations in the biomechanics of this joint can produce significant symptoms. Computerized tomography (CT) is best able to define the bony anatomy, and with thin sections, scanning reconstructions in the axial, coronal, and sagittal planes can be performed. Magnetic resonance imaging (MRI) can be used to confirm associated bony changes such as subchondral bone edema and may be useful in evaluating the adjacent soft tissues to rule out other causes of hindfoot pain. Bone scanning and arthrography are usually not required, and these studies have largely been replaced by MRI.
TREATMENT
Indications and Contraindications
The contraindications to arthroscopic subtalar arthrodesis include prior failed subtalar fusions, gross malalignment requiring correction, infection, and significant bone loss. A patient with moderate malalignment may be a candidate for in situ stabilization. Although significant bone loss has not frequently been encountered, moderate bone loss has not presented a serious problem in a study of arthroscopic ankle arthrodesis.15
Arthroscopic Technique
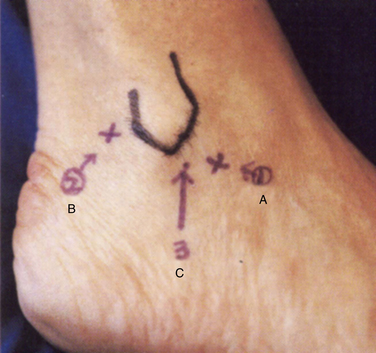
The anterolateral and the posterolateral portals are conventionally used. An accessory portal usually needs to be established approximately 1 cm posterior to the anterolateral portal (Fig. 18-4). This portal can be used for debridement or for outflow enhancement and may occasionally be used for visualization. The anterolateral and posterolateral portals are used in an alternating manner for viewing and for instrumentation. If significant arthrofibrosis makes entry and visualization difficult, the accessory anterolateral portal is quite useful.
Related posts:
 Osteochondral Lesions of the Talar Dome: Cartilage Replacement Using Osteochondral Autogenous Transplantation and Mosaicplasty
Osteochondral Lesions of the Talar Dome: Cartilage Replacement Using Osteochondral Autogenous Transplantation and Mosaicplasty
 Bony Impingement of the Ankle and Subtalar Joints
Bony Impingement of the Ankle and Subtalar Joints
 Osteochondral Lesions of the Talar Dome: D
Osteochondral Lesions of the Talar Dome: D
 Tendoscopy
Tendoscopy
 Fusion for Degenerative Arthritis of the Ankle
Fusion for Degenerative Arthritis of the Ankle
 Diagnostic Arthroscopy for the Ankle and Subtalar Joints
Diagnostic Arthroscopy for the Ankle and Subtalar Joints
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


